 |
Case Report
Riedel’s thyroiditis as a part of the IgG4 systemic disease: A case report
1 Endocrine Division, Hospital Universitário Pedro Ernesto, State University of Rio de Janeiro, Rio de Janeiro/RJ, Brazil
2 Postgraduate Program in Clinical and Experimental Pathophysiology (FISCLINEX), Faculty of Medical Sciences, State University of Rio de Janeiro, Rio de Janeiro/RJ, Brazil
3 Reumathology Division, Hospital Universitário Pedro Ernesto, State University of Rio de Janeiro, Rio de Janeiro/RJ, Brazil
4 Pathology and Cytopathology Laboratory, Microimagem, Rio de Janeiro/RJ, Brazil
5 MD, PhD, Endocrine Division, Hospital Universitário Pedro Ernesto, State University of Rio de Janeiro, Rio de Janeiro/RJ, Brazil
Address correspondence to:
Bárbara Gehrke
Boulevard 28 de Setembro, 77, Vila Isabel, Rio de Janeiro 20551-030,
Brazil
Message to Corresponding Author
Article ID: 101194Z01TM2021
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Marques T, Gehrke B, Ribeiro FM, Machado M, Romano SO, Coelho MCA. Riedel’s thyroiditis as a part of the IgG4 systemic disease: A case report Int J Case Rep Images 2021;12:101194Z01TM2021.ABSTRACT
Introduction: Riedel’s thyroiditis (RT) is a fibro-inflammatory process that can affect the thyroid gland alone or might extend to adjacent tissues. This condition may evolve to multifocal systemic fibrosclerosis in 30–40% of the patients. Riedel’s thyroiditis is a rare disease that is usually treated by surgery as it consists of a hardened, adhered goiter with local invasion that resembles a malignant lesion. This thyroid disease is considered the most associated to immunoglobulin G4-related disease (IgG4-RD). IgG4-RD is characterized by a dense lymphoplasmacytic infiltrate with numerous IgG4 positive plasma cells present in other organs besides the thyroid.
Case Report: The report refers to a 53-year-old female Brazilian patient. The patient had a medical history of hypothyroidism and also showed increase of the cervical volume since the beginning of 2018. A surgical treatment was proposed in 2019 and histological aspects suggested the diagnosis of RT. After further analysis of the material obtained in biopsy, the microscopy assessment revealed lymphoplasmacytic inflammation with high fibrosis suggesting IgG4 related sclerotic disease.
Conclusion: This case highlights the importance of investigating IgG4-RD in patients with RT as it seems to be a new clinical entity. The diagnosis is a challenge and the combination of histopathological features/immunohistochemical staining with clinical, laboratorial, and radiological findings is extremely important.
Keywords: Immunoglobulin G4-related disease, Retroperitoneal fibrosis, Sclerosis, Thyroiditis
Introduction
Riedel’s thyroiditis (RT) is characterized by a fibrotic and inflammatory process that spreads to tissues that surround the thyroid gland. It is an uncommon condition with prevalence of 1 in each 100,000 people, most frequent in females between 30 and 50 years [1]. According to Rotondi et al., Berhard Riedel first described RT in 1896, but only in 2010 Dalgren suggested the histologic diagnostic criteria, which included: fibro-inflammatory process involving all or a portion of the thyroid gland; presence of fibrous extension to thyroid capsule and adjacent tissues; inflammatory cells infiltration (without giant cells), lymphoid follicles, oncocytes or granulomas; presence of occlusive phlebitis and absence of a neoplasm [2].
Studies demonstrate that RT seems to be the thyroid condition most associated with immunoglobulin G4-related disease (IgG4-RD), that is characterized by dense lymphoplasmacytic infiltrate with numerous IgG4 positive plasma cells, and propensity to form tumefactive lesions and storiform fibrosis [2]. The diagnosis of this disease is a challenge due to the heterogeneity of its clinical presentation and variable diagnostic criteria.
Case Report
A 53-year-old woman, smoker (25 packs/year), carrier of hypothyroidism (diagnosed in 2015 with positive antibodies against thyroperoxidase), complaining of hoarseness, dysphagia and increase of cervical volume. Computed tomography (CT) of the cervical region (Figure 1) demonstrated a mass at the left base of the neck, heterogeneous, extending into the mediastinum, measuring 7.0×5.0×5.0 cm, encasing the common carotid artery and associated with thrombosis of the internal jugular vein at the same side. Magnetic resonance imaging (MRI) of cervical region showed a mass with isointense signal in T1 and hyperintense in T2, insinuating into the thoracic introit at the same side for approximately 2.7 cm, surrounding vascular structures, measuring 7.0×4.0×4.5 cm. The patient was treated by surgery and histological aspects suggested the diagnosis of Riedel’s thyroiditis: fibroblastic proliferation with inflammatory lymphoplasmacytic component replacing normal thyroid tissue and extending to striated muscle, with the presence of obliterating angiitis associated. Then, prednisone was initiated at dose of 20 mg. Abdominal CT and blood samples were requested due to possible association with IgG4-RD. No changes in bone metabolism, hepatic function, or IgG4 titer (Table 1) were observed.
Abdominal CT evidenced aorta with preserved caliber, presenting a thickening of parietal tissue, highlighting contrast from underneath the kidneys extending down to the common iliac artery to the left, suggesting retroperitoneal fibrosis. Computed tomography of cervical region eight months after prednisone evidenced lesion at topography of the thyroid gland to the left, measuring 6.7×4.2×3.1 cm. After further analysis of the material obtained through biopsy, microscopy examination revealed atrophic thyroid parenchyma and intense infiltrated lymphoplasmacytic inflammation with extensive fibrosis that extends up to muscular structures surrounding the thyroid, associated with obliterating angiitis, and also involving the parathyroid glands, suggesting IgG4 related sclerotic disease. IgG4 immunostaining with the ratio IgG4+/IgG+ ratio in tissue <10% (Figure 2).
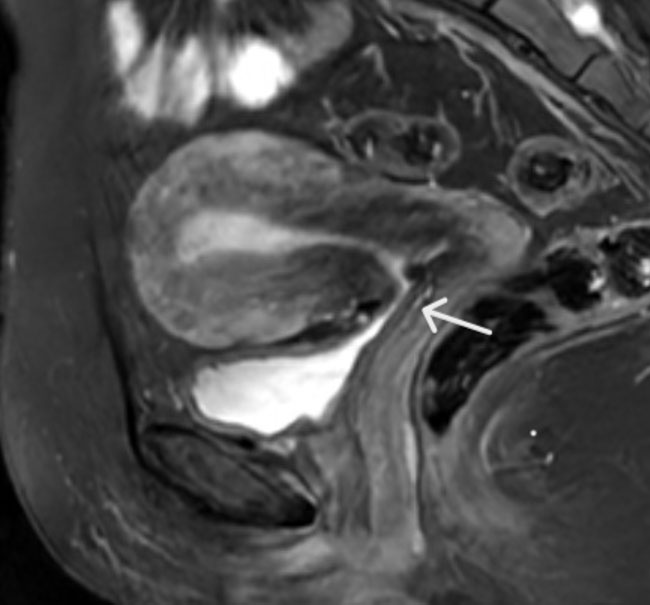
Magnetic resonance angiography of thoracic and abdominal aorta was requested in order to visualize the retroperitoneal fibrosis and to define the best therapeutic approach for RT associated to IgG4-RD. The exam demonstrated enhancing of periaortic tissue, approximately 0.7 cm thick, asymmetric, mainly on the anterior wall, located near the infrarenal aorta, suggestive of periaortitis (Figure 3). Unfortunately, glucocorticoid dosage could not be optimized due to diabetes onset after eight months of prednisone and patient refusal. At the moment patient is undergoing evaluation to initiate Rituximab therapy.




Discussion
IgG4-related disease is a new clinical entity, immune-mediated, characterized by lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells that can affect various organs, including the thyroid. It is an underdiagnosed disease with current prevalence of 6/100,000, peak incidence between 50 and 70 years of age and male predominance [2]. Riedel’s thyroiditis seems to be the thyroid disease with highest association to IgG4-RD, although the real prevalence of this association remains unknown [3].
Riedel’s thyroiditis can be associated with primary sclerosing cholangitis, orbital and mediastinal fibrosis, or with retroperitoneal fibrosis as described in this case report. Riedel’s thyroiditis can occur at the same time of the retroperitoneal fibrosis or years later, and when associated with RT there is a higher prevalence in females [2].
Riedel’s thyroiditis is suspected in the presence of fixed and hard neck mass. It can commonly manifest with obstructive symptoms such as dysphagia, hoarseness, and dyspnea due to involvement of structures adjacent to the thyroid gland. In addition, it may present symptoms of hypothyroidism or hypoparathyroidism [4]. In our case, similar to what is evidenced in literature, RT caused pressure symptoms due to an increase of the thyroid gland (dysphagia and hoarseness). Although hypothyroidism may be found in 1/3 of patients with RT, the diagnosis of hypothyroidism was prior to the onset of RT symptoms in our patient. Several cases of Hashimoto’s thyroiditis have been reported previously or concomitantly to RT. Usually the thyroid function is normal, although 90% of cases antibody titers against thyroglobulin (Tg-Ab) and thyroperoxidase (TPO-Ab) are elevated [5],[6]. Hypoparathyroidism may be a presenting symptom, because of its growth and compression, independent of surgical complications. However, our patient had normal laboratory levels of calcium and phosphorus.
There is a possible association of RT with smoking, which could be linked to a more aggressive course of the disease. Tobacco use may influence the immune response by activating fibrosis-related genes expression especially connective tissue growth factor, growth factor-β1, and interleukin-1β [7].
Imaging tests are not usually specific for the disease, but they can support the diagnosis. Ultrasound may present with low echogenicity of the thyroid gland, while CT shows a hypodense, infiltrative mass which enhances after contrast and MRI shows hypointensity in T1 and T2 images. In our patient, MRI showed expansive mass with isointense signal in T1 and hyperintense in T2, which differs from literature. Similar to previous reports, MRI has not added any new information compared to ultrasonography or CT. These findings explain why the diagnosis is not confirmed by imaging tests and usually requires a histopathological analysis to rule out malignant tumor [8],[9].
Anaplastic carcinoma, papillary carcinoma, lymphoma, fibrotic Hashimoto’s thyroiditis, and sarcoma of the thyroid are considered differential diagnosis of RT, as they may present clinical similarities, such as compressive symptoms due to gland growth [10],[11],[12]. Histological features of diffuse sclerosing papillary thyroid cancer may have resemblance to RT and should be ruled out [13].
The pathogenesis of the connection between RT and IgG4-RD is not yet known. In healthy subjects, IgG4 represents less than 5% of the total IgG and it seems to play a minor role in the IgG4-RD, since they are generally considered anti-inflammatory. There is no clear evidence if IgG4 participates in the pathogenesis or if it is a consequence of the process. Recent data defend the idea that an increase in IgG4 levels should be interpreted as an effort to reduce inflammation mediated by a given antigen [3].
The diagnosis of IgG4-RD is a challenge and for the definitive diagnosis the combination of histopathological features/immunohistochemical stain with clinical, laboratorial, and radiological findings suggestive of the disease is necessary. The laboratorial diagnosis is marked by an increase in IgG4 (normally over 135 mg/dL) blood levels and radiological findings consist of the involvement of other organs [2],[3].
The histopathological features are divided into major and minor criteria. For the diagnosis it is necessary 2 of the 3 major criteria: infiltrate rich with IgG4 cells; storiform aspect fibrosis and obliterative phlebitis. The minor criteria: phlebitis without obliteration and an increase in eosinophil levels alone are neither sensitive nor specific for the disease.
IgG4 immunostaining is an essential test for the pathological diagnosis of IgG4-RD. There is no cutoff for the number of IgG4+ plasma cells in the tissue to characterize the disease. This number appears to be tissue specific and depends on the amount of fibrosis at diagnosis. On biopsy specimens over 10 numbers of IgG4+ plasma cells per high-power field (hpf) is suggestive of IgG4-RD [14],[15].
However, several inflammatory lesions, lymphoma, and malignances may increase the number of IgG4+ plasma cells per hpf unrelated to IgG4-RD [16],[17]. In this case the IgG4+/IgG+ ratio seems to be better than the isolated IgG4+ dosage. Some authors suggest a 40% cutoff in the IgG4+/IgG+ ratio in any organ to document the disease in case of patients with histopathological features and a compatible clinical picture [18],[19]. Nevertheless, 40% of patients with biopsy-proven disease may have normal IgG4 serum levels [20].
The patient had retroperitoneal fibrosis on imaging and met two major histopathological criteria, which strongly suggested IgG4-RD. Yet, she had normal serum dosage of IgG4 and the ratio IgG4+/IgG+ ratio in tissue was < 10% at immunohistochemical. These results may be due to sampling artifact, use of corticosteroid during a long period (eight months) before the exam or progression to a fibrotic stage. Thus, in the absence of a more specific biomarker, the diagnosis is based primarily on the morphological appearance on biopsy. Tissue IgG4 count and IgG4+/IgG+ ratio seems to be of secondary importance [21].
Regarding treatment, there are no clinical trials due to the rare number of cases involving this disease. However, according to literature, the use of glucocorticoids constitutes the base of the initial treatment, but there is no consensus about dosage, ranging from 15 to 100 mg per day. The response to therapy is evidenced by reduction of lesion dimensions, with consequent relief of compressive symptoms [22],[23]. Our patient did not show reduction of cervical mass with 20 mg of prednisone and unfortunately this dose could not be increased due to the development of secondary diabetes. For this reason, another therapy had to be considered. The increment of fibrosis evidenced in late disease in comparison to early disease (with predominance of inflammation) could explain the non-response to glucocorticoids therapy [23],[24],[25].
Patients who do not present an acceptable response to corticosteroids or those who cannot use this medication for any other reason, may use tamoxifen as a second line treatment. It is a selective estrogen receptor modulator that stimulates tumor growth factor beta (TGF-β) which works as a powerful growth inhibitor, usually administrated around 10–20 mg two times daily [26]. Rituximab and micofenolate are immunosuppressive agents that may also be considered when treating RT associated to IgG4-GD. Both have anti-fibrotic features and are used in systemic fibrosis that do not respond to the drugs named above [27],[28].
The prognosis of RT is extremely variable, from mild to rapidly progressive forms and tracheal compression is the major cause of mortality (around 10%). Surgery may be considered in order to alleviate compressive symptoms and to rule out malignity, once it is very difficult to differentiate fibrotic tissue from normal thyroid gland during procedure [9].
Conclusion
Riedel’s thyroiditis is a rare condition, with prevalence higher in women and characterized by the appearance of goiter with compression of adjacent structures due to invasion of extra-thyroid tissues. Riedel’s thyroiditis seems to be the thyroid disease that is most associated to IgG4-RD, and for this reason it is important to actively investigate this association and accomplish a biopsy with histopathology analysis and laboratory evaluation. Though it is an uncommon disease and with limited cases reported in literature, a considerable amount of patients respond well to drug therapy, being surgery preferred only to relief compressive symptoms.
REFERENCES
1.
Hay ID. Thyroiditis: A clinical update. Mayo Clin Proc 1985;60(12):836–43. [CrossRef]
[Pubmed]

2.
Rotondi M, Carbone A, Coperchini F, Fonte R, Chiovato L. Diagnosis of endocrine disease: IgG4-related thyroid autoimmune disease. Eur J Endocrinol 2019;180(5):R175–83. [CrossRef]
[Pubmed]
3.
Kottahachchi D, Topliss DJ. Immunoglobulin G4-related thyroid diseases. Eur Thyroid J 2016;5(4):231–9. [CrossRef]
[Pubmed]
4.
Marín F, Araujo R, Páramo C, Lucas T, Salto L. Riedel's thyroiditis associated with hypothyroidism and hypoparathyroidism. Postgrad Med J 1989;65(764):381–3. [CrossRef]
[Pubmed]
5.
Graham A, Gilliland IC. Riedel's thyroiditis. Br Med J 1959;2(5146):225–6. [CrossRef]
[Pubmed]
6.
Zelmanovitz F, Zelmanovitz T, Beck M, Cerski CT, Schmid H, Czepielewski MA. Riedel's thyroiditis associated with high titers of antimicrosomal and antithyroglobulin antibodies and hypothyroidism. J Endocrinol Invest 1994;17(9):733–7. [CrossRef]
[Pubmed]
7.
Kau HC, Wu SB, Tsai CC, Liu CJL, Wei YH. Cigarette smoke extract-induced oxidative stress and fibrosisrelated genes expression in orbital fibroblasts from patients with Graves' ophthalmopathy. Oxid Med Cell Longev 2016;2016:4676289. [CrossRef]
[Pubmed]
8.
Ozgen A, Cila A. Riedel's thyroiditis in multifocal fibrosclerosis: CT and MR imaging findings. AJNR Am J Neuroradiol 2000;21(2):320–1.
[Pubmed]
9.
Fatourechi MM, Hay ID, McIver B, Sebo TJ, Fatourechi V. Invasive fibrous thyroiditis (Riedel thyroiditis): The Mayo Clinic experience, 1976–2008. Thyroid 2011;21(7):765–72. [CrossRef]
[Pubmed]
10.
Torres-Montaner A, Beltrán M, Romero de la Osa A, Oliva H. Sarcoma of the thyroid region mimicking Riedel's thyroiditis. J Clin Pathol 2001;54(7):570–2. [CrossRef]
[Pubmed]
11.
Won YS, Lee HH, Lee YS, et al. A case of Riedel's thyroiditis associated with benign nodule: Mimic of anaplastic transformation. Int J Surg 2008;6(6):e24–7. [CrossRef]
[Pubmed]
12.
Canos JC, Serrano A, Matias-Guiu X. Paucicellular variant of anaplastic thyroid carcinoma: Report of two cases. Endocr Pathol 2001;12(2):157–61. [CrossRef]
[Pubmed]
13.
Chung J, Lee SK, Gong G, et al. Sclerosing Mucoepidermoid carcinoma with eosinophilia of the thyroid glands: A case report with clinical manifestation of recurrent neck mass. J Korean Med Sci 1999;14(3):338–41. [CrossRef]
[Pubmed]
14.
Lindstrom KM, Cousar JB, Lopes MBS. IgG4-related meningeal disease: Clinico-pathological features and proposal for diagnostic criteria. Acta Neuropathol 2010;120(6):765–76. [CrossRef]
[Pubmed]
15.
Saeki T, Nishi S, Imai N, et al. Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis. Kidney Int 2010;78(10):1016–23. [CrossRef]
[Pubmed]
16.
Shimizu I, Nasu K, Sato K, et al. Lymphadenopathy of IgG4-related sclerosing disease: Three case reports and review of literature. Int J Hematol 2010;92(5):751–6. [CrossRef]
[Pubmed]
17.
Witkiewicz AK, Kennedy EP, Kennyon L, Yeo CJ, Hruban RH. Synchronous autoimmune pancreatitis and infiltrating pancreatic ductal adenocarcinoma: Case report and review of the literature. Hum Pathol 2008;39(10):1548–51. [CrossRef]
[Pubmed]
18.
Chen G, Cheuk W, Chan JKC. IgG4-related sclerosing disease: A critical appraisal of an evolving clinicopathologic entity. [Article in Chinese]. Zhonghua Bing Li Xue Za Zhi 2010;39(12):851–68.
[Pubmed]
19.
Sato Y, Kojima M, Takata K, et al. Systemic IgG4-related lymphadenopathy: A clinical and pathologic comparison to multicentric Castleman's disease. Mod Pathol 2009;22(4):589–99. [CrossRef]
[Pubmed]
20.
Sah RP, Chari ST. Serologic issues in IgG4-related systemic disease and autoimmune pancreatitis. Curr Opin Rheumatol 2011;23(1):108–13. [CrossRef]
[Pubmed]
21.
Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol 2012;25(9):1181–92. [CrossRef]
[Pubmed]
22.
Bozkirli E, Bakiner OS, Ersozlu Bozkirli ED, et al. Serum Immunoglobulin G4 levels are elevated in patients with Graves' ophthalmopathy. Clin Endocrinol (Oxf) 2015;83(6):962–7. [CrossRef]
[Pubmed]
23.
Vaidya B, Harris PE, Barrett P, Kendall-Taylor P. Corticosteroid therapy in Riedel's thyroiditis. Postgrad Med J 1997;73(866):817–9. [CrossRef]
[Pubmed]
24.
Bagnasco M, Passalacqua G, Pronzato C, Albano M, Torre G, Scordamaglia A. Fibrous invasive (Riedel's) thyroiditis with critical response to steroid treatment. J Endocrinol Invest 1995;18(4):305–7. [CrossRef]
[Pubmed]
25.
Thomson JA, Jackson IM, Duguid WP. The effect of steroid therapy on Riedel's thyroiditis. Scott Med J 1968;13(1):13–6. [CrossRef]
[Pubmed]
26.
Butta A, MacLennan K, Flanders KC, et al. Induction of transforming growth factor beta 1 in human breast cancer in vivo following tamoxifen treatment. Cancer Res 1992;52(15):4261–4.
[Pubmed]
27.
Levy JM, Hasney CP, Friedlander PL, Kandil E, Occhipinti EA, Kahn MJ. Combined mycophenolate mofetil and prednisone therapy in tamoxifen- and prednisone-resistant Reidel's thyroiditis. Thyroid 2010;20(1):105–7. [CrossRef]
[Pubmed]
28.
Carruthers MN, Topazian MD, Khosroshahi A, et al. Rituximab for IgG4-related disease: A prospective, open-label trial. Ann Rheum Dis 2015;74(6):1171–7. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Thamyres Marques - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bárbara Gehrke - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Francinne Machado Ribeiro - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Marise Machado - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Sérgio de Oliveira Romano - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Maria Caroline Alves Coelho - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2021 Thamyres Marques et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}