 |
Case Report
Esthetic rehabilitation with porcelain crowns using digital planning
1 Professor, Department of Restorative Dentistry, University of Santo Amaro, São Paulo, SP, Brazil
2 Master Student, Department of Biological Sciences, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil
3 PhD, Department of Restorative Dentistry, Piracicaba Dental School, University of Campinas, Campinas, SP, Brazil
4 Adjunct Professor, Department of Dentistry, Faculty of Sciences of Health, Federal University of Jequitinhonha and Mucuri Valley, Diamantina, MG, Brazil
5 Master Student, Department of Dental Clinic, Federal University of Piauí, Teresina, PI, Brazil
6 DDS, Gama Filho University, Rio de Janeiro, RJ, Brazil
7 Professor, Department of Dental Clinic, School of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil
Address correspondence to:
João Victor Frazão Câmara
Alameda Doutor Octávio Pinheiro Brisolla, 6-65, CEP 17012-059, Bauru, São Paulo,
Brazil
Message to Corresponding Author
Article ID: 101168Z01JP2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Pierote JJA, Câmara JVF, Barbosa IF, de Araújo CTP, Carvalho GAO, de Castro AN, Pereira GDS, Prieto LT. Esthetic rehabilitation with porcelain crowns using digital planning. Int J Case Rep Images 2020;11:101168Z01JP2020.ABSTRACT
Introduction: The desire for a perfect smile has increased substantially over the past few years. After the esthetic dental treatment, patients seem more confident and happy, which results in greater chances of success in job interviews and better personal relationships.
Case Report: A male patient, sought dental care, reporting smile esthetics as the main complaint. After clinical and radiographic evaluations, tooth wear was observed on central and lateral incisors due to dental erosion. A photographic protocol was performed for digital planning and then, from the diagnostic wax-up, a mold was made with addition silicone and bis-acrylic resin was used for the mock-up. The minimally invasive preparation was carried out with diamond burs of fine and ultrafine granulations and consisted in the removal of the live angles and retentive areas. The crowns were made in lithium disilicate (LD) glass-ceramic, following the treatment protocol with hydrofluoric acid, phosphoric acid, adhesive, and a cementing agent. The excess was removed and photoactivation was performed for 40 seconds on the buccal, lingual, and incisal surfaces on each tooth and subsequent finishing and polishing.
Conclusion: The clinical success of lithium disilicate porcelain crowns depends on the precise clinical protocol, correct indications, and laboratory procedures.
Keywords: Dental porcelain, Lithium, Mouth rehabilitation
Introduction
The desire for a perfect smile has increased substantially over the past few years. After the esthetic dental treatment, patients seem more confident and happy, which results in greater chances of success in job interviews and better personal relationships. The esthetic restoration of anterior teeth intends to provide a healthy and harmonious smile, solving some of the most esthetic problems for patients: size, shape, and color of anterior upper teeth. The options to solve these problems range from composite resins to ceramics and each one presents advantages and limitations [1],[2].
Composite resin is one of the most commonly used materials in dental practice, mainly because it preserves more dental tissue, costs less than ceramics, and it presents reversibility and a relatively simple technique [3]. However, such restorations have limited longevity, which compromises the long-term esthetic results [4]. Therefore, the material of choice for patients with high esthetic expectations and seeking a long-lasting treatment have been ceramics [3].
Feldspathic porcelains have properties similar to those of metallic alloys, for example, when incorporating leucite to increase the coefficient of thermal expansion and minimize thermal stress superior [3]. Moreover, esthetics are used for making inlay and onlay crowns, dental veneers, anterior partial crowns, posterior crowns, bridges in three anterior units and bridges and implant super structures until the second pre-molar. As an example of free material, there is a system based on glassy ceramic of lithium disilicate (LD), characterized by presenting crystals of LD densely arranged and joined to the glass matrix [3],[5]. This type of material is widely used in dental clinical practice because it combines advantages that allow its indication, such as, esthetic properties of natural teeth, durability, resistance, biocompatibility, and translucency, and as they are characterized as thin structures, they minimize wear on the tooth structure during preparation. Considering the increasing demand for esthetic restorations, the use of IPS e.max Press, a relatively translucent high-strength monolithic ceramic material, is rather popular [6].
Thus, we present a case of restoration of esthetics and harmony of the patient’s smile using LD porcelain crowns.
Case Report
A male patient, sought dental care, reporting smile esthetics as the main complaint. After clinical and radiographic evaluations, without pulp alteration, tooth wear was observed on central and lateral incisors due to dental erosion (Figure 1A, Figure 1B, Figure 1C).
After discussing with the patient about treatment modalities, we decided to restore the size and shape of the teeth with LD crowns. The composite resin was not used, as the patient had already undergone this treatment and observed that this material pigments rapidly. To initiate the treatment, oral adequacy was performed with the supragingival scaling of calculi with periodontal curettes and root planting with rubber cups in low rotation and water paste/pumice.
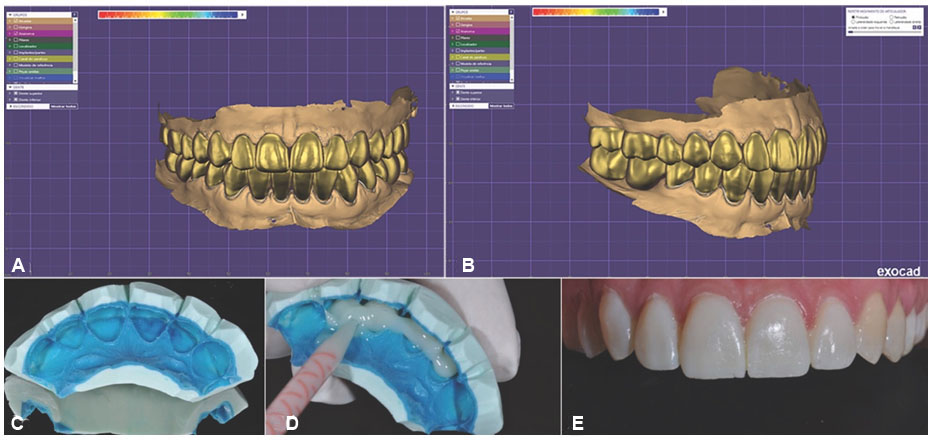
The dental arches were cast with a scanner (iTero Element, iTero Intraoral Scanner, USA) to obtain the dental template. The case was planned with a digital planning software (Exocad, Exocad GmbH, Germany) (Figure 2A and Figure 2B). The software’s user interface provides a highly interactive 3D modeling experience, allowing to maximize the productivity and reduce training costs. The CEREC system uses a chain of processes that consist of the stages of scanning, anatomization, and milling. The scan converts the prepared tooth into a 3D image (Voxels), which is sent to the computer for the anatomical definition of the piece. Once the anatomy is completed, the milling unit makes the restoration using the chosen restorative material. Thus, impressions were obtained and used for temporary restorations (Figure 2C and Figure 2D).
Finally, temporary restorations were produced with an acrylic resin (Vipi, Dental Vipi, Pirassununga, Brazil) (Figure 2E). The dental structure was removed for tooth preparation with a conical diamond bur (KG Sorensen, São Paulo, Brazil). To create a separation between the teeth in the proximal area, a metal sandpaper (KG Sorensen) was used to facilitate the definition of the proximal margin. Lastly, all angles were rounded, and an extra-thin and round conical bur (KG Sorensen) was used to smooth the prepared surface (Figure 3A, Figure 3B, Figure 3C).
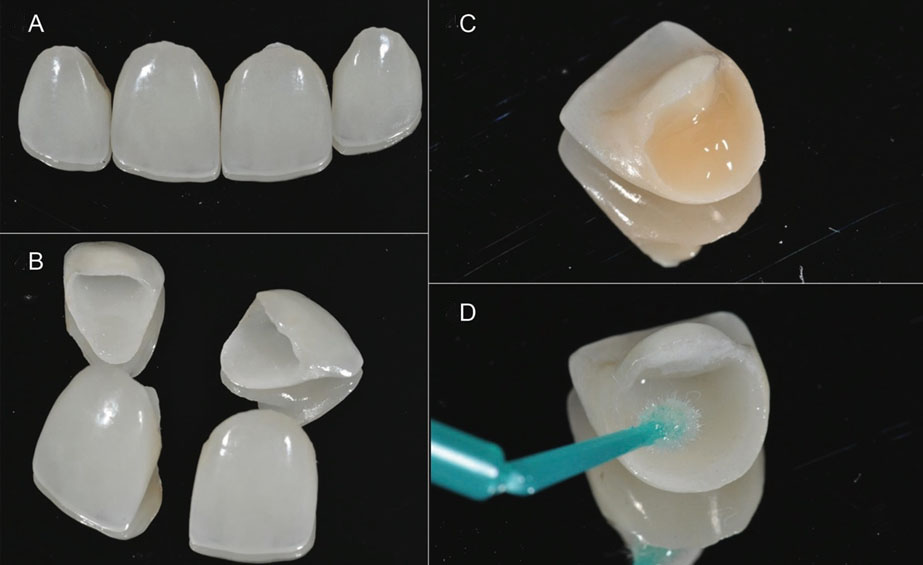
The crowns were made of LD (Emax Esthetic, IvoclarVivadent, São Paulo, Brazil). After a technician produced the crowns (Figure 4A and Figure 4B), they were carefully positioned to check the marginal fit, alignment, shape, and color, with completely satisfactory results. The gingiva and the prepared tooth were isolated before the prophylaxis of the teeth with pumice stone and rubber cup and then they were rinsed and thoroughly washed. The internal conditioning of the restorations was performed for one minute, applying 10% hydrofluoric acid (Condac Porcelana, FGM Products) (Figure 4C), washing with water, and air drying. Subsequently, the silane agent (RelyX Ceramic Primer, 3M ESPE) was applied and the surface was gently air-dried (Figure 4D). The crowns were shrunk for each tooth individually, following the same sequence for each one. The teeth were etched with 37% phosphoric acid (Condac 37, FGM Products) for 30 seconds, rinsed, and carefully dried. Next, a one-bottle bonding system (Single Bond, 3M ESPE) was applied and the surface was gently air-dried and polymerized for 40 seconds.
The cementing agent RelyX Veneer B1 resin cement (3M ESPE, São Paulo, Brazil) was applied to the inner surface of the crown and then positioned. After light curing for 5 seconds, excess cement was removed using hand instruments and the crown was again light-cured on the buccal and palatine surfaces for 40 seconds.
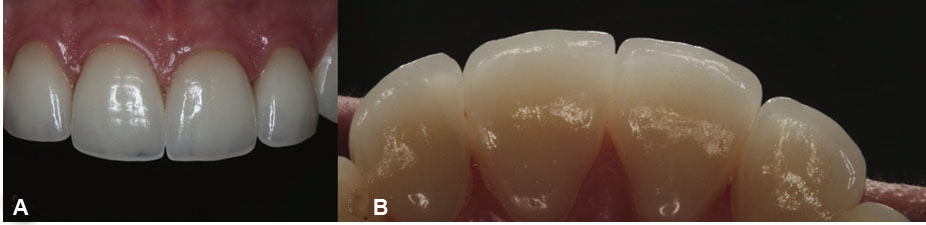
After placing the entire crown, the cervical margins were verified and the excess cement was removed with sandpaper strips. The cement line was finished and polished with a silicone rubber (Resin Finish, Microdont) and a silicon carbide brush (Jiffy Brush, Ultradent). The result could be seen in a 1-month clinical follow-up with intraoral aspects of the patient (Figure 5A and Figure 5B).


Discussion
In this case report, the patient’s main complaint was the size, color, and shape of upper anterior teeth and the treatment possibilities were discussed, including composite resin or ceramic crowns. The patient chose the ceramic crown treatment because of their short-term color stability and their low wear resistance, as the patient aimed for a long-lasting result.
Diagnostics are essential for a predictable treatment outcome in esthetic dentistry. Therefore, a diagnostic wax-up was performed for better communication between the patient, clinician, and the technician. This procedure allows the dentist to perform the mock-up technique, which is useful for patients to visualize their smiles and the integration of gum, lips, and face. Thereafter, the patient was able to evaluate the results expected, express an opinion, and approve the final shape of the smile [4],[7].
The porcelain crown, when produced in combination with a precise clinical protocol and correct indications, offers excellent longevity and esthetics [3]. The crown exhibits a natural fluorescence and absorbs, reflects, and transmits light exactly as a natural tooth [8].
According to Sieper et al. [7], the fracture strength of LD crowns compared to polymer-infiltrated ceramic-network and zirconia-reinforced lithium silicate crowns was above the clinically expected loading forces. This reinforces the indication of this material in the rehabilitation of patients due to its durability. Another study that evaluated 318 anterior veneers made of silicate glass-ceramic cemented with different types of cements in 84 patients observed an approximately 93.5% survival rate over 10 years [3].
An important step to achieve clinical success is to select an appropriate ceramic material for each case. There are many types of ceramics and each one is different due to the brand, as well as thickness, color, translucency, opalescence, fluorescence, surface texture, and shape [9].
Lithium disilicate glass-ceramic is composed of 65% LD, which results in a relatively strong ceramic with a high flexural strength of about 400 MPa and fracture toughness of 3.3 MPa m0.5, and both values are approximately higher than the IPS empress 2 [6],[10]. In a study, 74 anterior crowns and 20 posterior crowns made with LD (IPS-e.max) were evaluated and had a survival rate of 97.4% after five years and 94.8% after eight years of clinical service [11].
The LD system has a very clear translucency property that allows light to reflect, due to the low refractive index of the crystals. This characteristic also allows the use of the material for the manufacture of monolithic restorations, with a completely anatomical and integral contour. In addition, the color of the material can be controlled by adding or dissolving polyvalent ions inside the glassy ceramic and the flexural strength is associated with the volume and shape of the crystals [12].
Masticatory tension, proven saliva water and dentinal tubules, thermal changes, and pH are factors that cause failure in the ceramic material. Ferruzi and collaborators evaluated the ways of resistance to fatigue and damage of posterior monolithic nanoceramic resin and ceramic crowns of LD. The results showed that in the different damage modes, both materials had the potential to cause mass fracture failure [13].
The durability of the bond between tooth and restoration depends on the chemical composition of the adhesive and luting agents and the surface treatment of laminates [14]. Interfacial fracture toughness for the LD glass-ceramic system is affected by the surface treatment and type of luting agent [15]. However, the composite resin bonded to etched porcelain, both with silane alone or silane with dentin adhesive, produces high shear bond strengths [14]. The bond strength of hydrofluoric acid-etched and silanized veneer to the luting resin composite is generally higher than the bond strength of the same luting resin to the etched enamel surface [8].
The computer-aided design (CAD)/computer-aided manufacturing (CAM) system is a revolutionary technology in dentistry, as it allows ceramic restorations to be performed in the dental office through a milling machine, combining the benefits of direct restorations [16]. The first commercially viable CAD/CAM system was CEREC, developed by Mörmann and Brandestini [17]. The advantages are: excellent adaptation and longevity, the use of new materials with adequate mechanical properties, reduction of the operator’s impact on the final quality of work, completion of treatment in a single consultation, reduction of pulp stress resulting from excessive drying, cleaning, and trauma, in addition to the lack of need for molding, making provisionals, and paying for the laboratory. However, the initial cost to acquire the system and initial training can be considered as disadvantages. However, in the long run, large-scale production would supply the initial investment [16].
Dual-polymerizing resin cements contain aromatic tertiary amine and their oxidation could compromise the color stability of cemented restorations. Then, in vitro studies have indicated that light-polymerizing cements have excellent color stability due to the absence of this amine. These types of cements also have a longer working time compared to chemically and dual-cured cements, which makes it easier to remove any excess material before light-curing [5].
Conclusion
In this case, the use of LD glass-ceramic was an excellent alternative in cases of previous teeth with shape change, mainly because veneers exhibit natural fluorescence and absorb, reflect, and transmit light exactly as a natural tooth. However, we highlight that, to achieve this result, a detailed planning with a good communication between patient, dentist, and the dental technician, as well as the correct selection of dental materials were essential.
REFERENCES
1.
Martins AV, Albuquerque RC, Santos TR, et al. Esthetic planning with a digital tool: A clinical report. J Prosthet Dent 2017;118(6):698–702. [CrossRef]
[Pubmed]

2.
Pithon MM, Nascimento CC, Barbosa GCG, da Silva Coqueiro R. Do dental esthetics have any influence on finding a job? Am J Orthod Dentofacial Orthop 2014;146(4):423–9. [CrossRef]
[Pubmed]
3.
Farias-Neto A, da Cunha Gomes Ferreira EM, Sánchez-Ayala A, Sánchez-Ayala A, Vilanova LSR. Esthetic rehabilitation of the smile with no-prep porcelain laminates and partial veneers. Case Rep Dent 2015;2015:452765. [CrossRef]
[Pubmed]
4.
Federizzi L, Gomes ÉA, Báratro SSP, Baratto-Filho F, Bacchi A, Spazzin AO. Use of feldspathic porcelain veneers to improve smile harmony: A 3-year follow-up report. Braz Dent J 2016;27(6):767–74. [CrossRef]
[Pubmed]
5.
Marchionatti AME, Wandscher VF, May MM, Bottino MA, May LG. Color stability of ceramic laminate veneers cemented with light-polymerizing and dual-polymerizing luting agent: A split-mouth randomized clinical trial. J Prosthet Dent 2017;118(5):604–10. [CrossRef]
[Pubmed]
6.
Yang Y, Yu J, Gao J, et al. Clinical outcomes of different types of tooth-supported bilayer lithium disilicate all-ceramic restorations after functioning up to 5 years: A retrospective study. J Dent 2016;51:56–61. [CrossRef]
[Pubmed]
7.
Sieper K, Wille S, Kern M. Fracture strength of lithium disilicate crowns compared to polymer-infiltrated ceramic-network and zirconia reinforced lithium silicate crowns. J Mech Behav Biomed Mater 2017;74:342–8. [CrossRef]
[Pubmed]
8.
Viswambaran M, Londhe SM, Kumar V. Conservative and esthetic management of diastema closure using porcelain laminate veneers. Med J Armed Forces India 2015;71(Suppl 2):S581–5. [CrossRef]
[Pubmed]
9.
Hernandes DKL, Arrais CAG, de Lima E, Cesar PF, Rodrigues JA. Influence of resin cement shade on the colour and translucency of ceramic veneers. J Appl Oral Sci 2016;24(4):391–6. [CrossRef]
[Pubmed]
10.
Zandinejad A, Lin WS, Atarodi M, Abdel-Azim T, Metz MJ, Morton D. Digital workflow for virtually designing and milling ceramic lithium disilicate veneers: A clinical report. Oper Dent 2015;40(3):241–6. [CrossRef]
[Pubmed]
11.
Zarone F, Ferrari M, Mangano FG, Leone R, Sorrentino R. “Digitally oriented materials”: Focus on lithium disilicate ceramics. Int J Dent 2016;2016:9840594. [CrossRef]
[Pubmed]
12.
Kurtzman GM, Ouellet DF. Evolution of comprehensive care, part 6: Aesthetics, veneers, and whitening. Dent Today 2016;35(1):24–9.
[Pubmed]
13.
Alavi AA, Behroozi Z, Nik Eghbal F. The shear bond strength of porcelain laminate to prepared and unprepared anterior teeth. J Dent (Shiraz) 2017;18(1):50–5.
[Pubmed]
14.
Lambade DP, Gundawar SM, Radke UM. Evaluation of adhesive bonding of lithium disilicate ceramic material with duel cured resin luting agents. J Clin Diagn Res 2015;9(2):1–5. [CrossRef]
[Pubmed]
15.
Hooshmand T, Rostami G, Behroozibakhsh M, Fatemi M, Keshvad A, van Noort R. Interfacial fracture toughness of different resin cements bonded to a lithium disilicate glass ceramic. J Dent 2012;40(2):139–45. [CrossRef]
[Pubmed]
16.
Fasbinder DJ. Clinical performance of chairside CAD/CAM restorations. J Am Dent Assoc 2006;137 Suppl:22S–31. [CrossRef]
[Pubmed]
17.
Mörmann WH. The evolution of the CEREC system. J Am Dent Assoc 2006;137 Suppl:7S–13. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Josué Junior Araújo Pierote - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
João Victor Frazão Câmara - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Isabel Ferreira Barbosa - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Cíntia Tereza Pimenta de Araújo - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guereth Alexsanderso Oliveira Carvalho - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Adriano Nóbrega de Castro - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gisele Damiana da Silveira Pereira - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lucia Trazzi Prieto - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Josué Junior Araújo Pierote et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}