 |
Case Report
Appendicular foreign body contributing to intestinal perforation
1 Department of General Surgery, West Hertfordshire Hospitals NHS Trust, Vicarage Road, Watford WD18 0HB, UK
Address correspondence to:
Sherif Monib
Department of General Surgery, West Hertfordshire Hospitals NHS Trust, Vicarage Rd, Watford WD18 0HB,
UK
Message to Corresponding Author
Article ID: 101165Z01SM2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Monib S, Amr B, Anis K, Zuberi J. Appendicular foreign body contributing to intestinal perforation. Int J Case Rep Images 2020;11:101165Z01SM2020.ABSTRACT
Introduction: Accidental foreign body ingestion is commonly encountered in clinical practice. Foreign bodies in the appendix are also well recognized but are very uncommon, as the majority of the ingested foreign bodies pass through the whole gastrointestinal tract without complications. Acute appendicitis due to a foreign body is a diagnostic dilemma; for which computed tomography is considered the method of choice for preoperative diagnosis.
Case Report: We are presenting a case of a 49-year-old gentleman who had small bowel perforation due to appendicular foreign body which initially presented with a clinical picture of acute appendicitis.
Conclusion: The low index of suspicion and prompt action are needed to reach a favorable outcome.
Keywords: Appendicitis, Foreign body, Perforation, Small bowel
Introduction
Bowel perforation due to a foreign body is uncommon, as the majority of foreign bodies uneventfully pass to the feces and only 1% of them (the sharper and more elongated objects) will perforate the gastrointestinal tract, usually at the level of the ileum [1].
Klingler et al. reported that ingested foreign bodies account for 0.0005% of the etiology of acute appendicitis [2]. Sharp pointed objects such as toothpicks, pins, needles, nails, and screws lead to perforation; however, other foreign bodies such as fish bones, chicken bone, swallowed tooth, thread, chewing gum, are usually causes of appendicitis and perforation [2], [3], [4]. Computed tomography (CT) is considered the method of choice for preoperative diagnoses of ingested foreign bodies and their complications due to its high-quality and high-resolution images [5],[6]. The increased availability and effectiveness of CT have limited the use of ultrasonography in investigations of acute abdominal pain. In the case report section, we made our diagnosis based on the CT findings.
Case Report
We are presenting a case of a 49-year-old gentleman who came to the Accident and Emergency Department complaining of central and abdominal pain, reduced appetite, and nausea. He also had a fever of four days duration; there was no change in bowel habits, rectal bleeding, or any genitourinary symptoms. His past medical history and family history were irrelevant. General examination was unremarkable, pulse rate was 115 BPM regular, blood pressure was 145/96 mmHg, temperature was 38.3 °C, and the respiratory rate was 20/minute. Abdominal examination revealed soft abdomen with tenderness at the epigastrium, localized guarding but no rebound tenderness and bowel sounds were normal; rectal examination revealed empty rectum, no bleeding or masses were found.
Laboratory investigations showed hemoglobin of 13.4 g/dL, white blood cell count 12.5 × 109/L, and serum amylase 32 U/L. Liver, renal function tests, and serum electrolytes were within normal limits. Plain abdominal X-rays showed no gas under the right hemidiaphragm or gas-fluid level. The patient was admitted with a provisional diagnosis of gastritis. He was kept nil by mouth, on intravenous fluids, and intravenous proton pump inhibitors (PPIs). Esophagogastroduodenoscopy (EGD) was carried out on the following day, which did not reveal any abnormality. Ultrasound scan (US) of the abdomen and pelvis revealed distended gall bladder with normal wall thickness, a small amount of sludge, but no calculi identified, it also showed thickened small bowel loops in the lower abdomen with increased echogenicity, but no free fluid in the abdomen and pelvis.
Two days later he had a temperature spike to 38.5 °C and his white blood cell count increased to 20 × 109/L, with no change in abdominal signs, he was started on intravenous antibiotic, and abdominopelvic CT scan with contrast was carried out which confirmed localized perforation in the terminal ileum with free fluid and air associated with marked increase inflammatory change in the mesenteric fat with associated lymphadenopathy, at the lower aspect of these changes, a V-shaped calcified foreign body was noted (Figure 1).
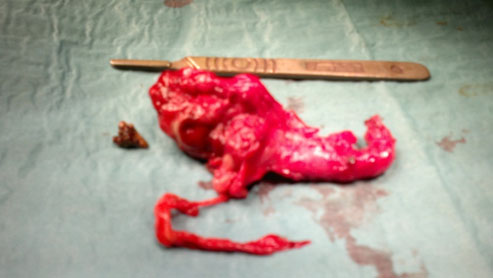
A midline laparotomy revealed, a long post ileal appendix passing through the mesentery, perforated at the tip into the wall of the ileum, with a chicken bone near the perforation. Small bowel loops and omentum surrounded the perforation site with minimal purulent fluid at the right iliac fossa (Figure 2). A limited right hemicolectomy with side to side anastomosis was carried out.
The patient had an uneventful recovery and was discharged on the six post-operative day, and seen in the clinic six weeks after with no complications noted.

Discussion
Although ingestion of an indigestible foreign body is frequent and is mostly a harmless event; intestinal perforation, as a result, is relatively rare. Most foreign bodies pass through the gastrointestinal tract without complications, with less than 1% resulting in perforation; those that cause perforation are usually either sharp or elongated [7],[8]. Foreign bodies in the appendix are very uncommon, with one study showing a frequency of 0.005% in 13,228 patients [9]. The literature has described many causes of foreign bodies in the appendix, such as seeds, needles, tongue studs, parasitic worms, bullets, and dental drill pieces [2],[10]. Madrona et al. reported that chicken bones are the most common foreign bodies causing gastrointestinal tract perforation [1]. While the ileum is the most common site of perforation, clinical presentations vary, depending on the site of perforation and the extent of peritonitis. Clinically, preoperative diagnosis of foreign body ingestion is a clinical challenge because ingestion is usually incidental and thus forgotten and unreported during a patient’s history assessment, which makes the clinical diagnosis more challenging, and a correct diagnosis is frequently delayed. The effectiveness of abdominal radiography in detecting an ingested foreign body depends on the size and radiodensity of the object [11]. Although chicken bones may be sufficiently radio dense to be seen on radiographs, they may be obscured by other bowel contents or overlying structures. On CT scans, foreign bodies, including bone, metal, and wood, are more readily detected. With gross perforation, free intra-peritoneal gas may be seen on radiographs. Computed tomography is more sensitive in detecting loculated extra-luminal gas or small amounts of free gas; CT is also better for localizing the site of perforation. In recent years, the availability of multi-detector-row computed tomography (MDCT) has resulted in its greater use in emergency departments. It has limited the use of US in the evaluation of acute abdomen cases; the high performance of CT or MDCT scan of the abdomen in identifying intestinal perforation caused by foreign bodies has been well described by Coulier et al. [12]. Multi-detector-row computed tomography is considered the method of choice for the evaluation of patients with acute abdominal pain and the depiction of foreign bodies due to its high-resolution, thin-collimation, multi-planar reconstructions, which allow the gastrointestinal tract to be examined in all projections. The final diagnosis and treatment for the perforation by a foreign body is surgical exploration and repair.
Conclusion
Although most ingested foreign bodies pass through the gastrointestinal tract without incident, perforation is still a possible complication, with disastrous consequences. These foreign bodies may lodge anywhere in the gastrointestinal tract, from the level of the esophagus to the rectum. Patients often do not recall ingesting the object, which makes the clinical diagnosis more challenging. The low index of suspicion and prompt action will lead to a favorable outcome.
REFERENCES
1.
Madrona AP, Fernández Hernández JA, Carrasco Prats M, Riquelme Riquelme J, Parrila Paricio P. Intestinal perforation by foreign bodies. Eur J Surg 2000;166(4):307–9.
[Pubmed]

2.
Klingler PJ, Seelig MH, DeVault RK, et al. Ingested foreign bodies within the appendix: A 100-year review of the literature. Dig Dis 1998;16(5):308–14. [CrossRef]
[Pubmed]
3.
Green SM, Schmidt SP, Rothrock SG. Delayed appendicitis from an ingested foreign body. Am J Emerg Med 1994;12(1):53–6. [CrossRef]
[Pubmed]
4.
Balch C, Silver D. Foreign bodies in the appendix: Report of eight cases and review of the literature. Arch Surg 1971;102(1):14–20. [CrossRef]
[Pubmed]
5.
Gonzalez JG, Gonzalez RR, Patiño JV, Garcia AT, Alvarez CP, Pedrosa CS. CT findings in gastrointestinal perforation by ingested fish bones. J Comput Assist Tomogr 1988;12(1):88–90. [CrossRef]
[Pubmed]
6.
Goh BKP, Tan YM, Lin SE, et al. CT in the preoperative diagnosis of fish bone perforation of the gastrointestinal tract. AJR Am J Roentgenol 2006;187(3):710–4. [CrossRef]
[Pubmed]
7.
Ziter FM Jr. Intestinal perforation in adults due to ingested opaque foreign bodies. Am J Gastroenterol 1976;66(4):382–5.
[Pubmed]
8.
Maleki M, Evans WE. Foreign-body perforation of the intestinal tract. Report of 12 cases and review of the literature. Arch Surg 1970;101(4):475–7. [CrossRef]
[Pubmed]
9.
Attia MW. The Paediatric Appendicitis Score (PAS) was useful in children with acute abdominal pain. Evid Based Med 2009;14(1):26. [CrossRef]
[Pubmed]
10.
Fischer CD, Mukherjee A. Appendicitis due to tongue stud ingestion: A case study and review of management plans. S D J Med 2004;57(1):19–22.
[Pubmed]
11.
Macmanus JE. Perforations of the intestine by ingested foreign bodies. Report of two cases and review of the literature. Am J Surg 1941;53(3):393–402. [CrossRef]
12.
Coulier B, Tancredi MH, Ramboux A. Spiral CT and multidetector-row CT diagnosis of perforation of the small intestine caused by ingested foreign bodies. Eur Radiol 2004;14(10):1918–25. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Sherif Monib - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Bassem Amr - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Karim Anis - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jamal Zuberi - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Sherif Monib et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}