 |
Case Report
Single-sided deafness related to neural vascular conflict: A case report from Saudi Arabia
1 Consultant, Head of Audio Vestibular Medicine Division, Department of ORL H & N Surgery, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Address correspondence to:
Mona S Al Rakaf
MD, MSc, AuD, Consultant, Head of Audio Vestibular Medicine Division, Department of ORL H & N Surgery, Prince Sultan Military Medical City, P.O. Box 7897, Riyadh 11159,
Saudi Arabia
Message to Corresponding Author
Article ID: 101150Z01MR2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Al Rakaf MS. Single-sided deafness related to neural vascular conflict: A case report from Saudi Arabia. Int J Case Rep Images 2020;11:101150Z01MR2020.ABSTRACT
The impact of single-sided deafness (SSD) is well known, particularly on children. These include difficulties in speech comprehension with background noise, localization, and spatial appreciation. The social and emotional status of the child may be compromised. In addition, parents are keen to understand the etiology and consequences of SSD. Different etiologies are correlated with SSD, and etiology identification is a crucial step toward better management and parent counseling. SSD related to neural vascular conflict (NVC) of the cerebellopontine angle is uncommon. This is the first case, up to my knowledge so far, to be reported in Saudi Arabia. A 13-year-old Saudi girl presented with a history of difficulty in hearing in the left ear, and audiological evaluation demonstrated left-sided profound sensorineural hearing loss. Upon further investigation, magnetic resonance imaging (MRI) showed a left-sided neural vascular conflict of the anterior inferior cerebellar artery (AICA) loop and the left cochlear nerve. In this case, SSD was related to NVC since clinical history, and other investigations did not justify another cause. This report will embrace the role of audiological and radiological investigation, which in turn will help with management recommendations, and help clinicians in dealing with similar challenges.
Keywords: Bone conduction hearing devices, Cochlear implantation, Neural vascular conflict, Single-sided deafness
Introduction
Single-sided deafness (SSD) in children is a condition in which they have a non-functional hearing in one ear and normal hearing in the contralateral ear. Individuals with bilaterally normal hearing have a tendency to comprehend speech in noise and have the ability to localize sound precisely [1]. The impact of SSD is well known, particularly in children. Consequences include: difficulties in comprehension speech with background noise, localization, and spatial appreciation. Furthermore, compromised competency of verbal communication and cognitive capacity affected academic performance, and incapacitated social and emotional status [2],[3]. In addition, patients with SSD will experience one-sided auditory deprivation, which will initiate neural plasticity within the auditory cortex and other sensory and cognitive areas [4].
Causes of SSD are congenital cytomegalovirus, meningitis, related syndromes, absence of the cochlear nerve, inner ear abnormality, acoustic neuroma, autoimmune diseases, chronic ear infection, and head trauma [5]. Neural vascular conflict (NVC) of the cerebellopontine angle is considered a rare cause of SSD among children, which can affect the V, VII, VIII, and IX cranial nerves. The commonest presenting symptom of NVC is trigeminal neuralgia, and next to that is hemifacial spasm [6]. Neural vascular conflict of the VIII nerve may provoke symptoms of tinnitus, hearing loss, and vertigo as neurotological symptoms. It was reported that after five centuries of investigations, the exact mechanisms beyond the pathogenesis of NVC are still undetermined [7]. Neurological signs related to the pressure effect of vascular loops within the cerebellopontine angle (CPA) on cranial nerves have been documented [8]. Etiological investigations for bilateral sensorineural hearing loss (SNHL) is more toward genetic causation. On the other hand, the temporal bone structural defect is more related to SSD [9]. According to a meta-analysis which composed of five case controls, NVC was significantly associated with SSD [10]. Moreover, 91 patients who were studied retrospectively for unexplained unilateral hearing loss or tinnitus had a negative clinical workup, NVC with MRI confirmation could be the culprit [11]. In this case, MRI showed a left-sided NVC of the AICA loop and the left cochlear nerve. Single-sided deafness was related to NVC in view of the fact that clinical history and other investigations did not justify another cause. In addition, the right side revealed normal hearing and negative MRI findings.
Case Report
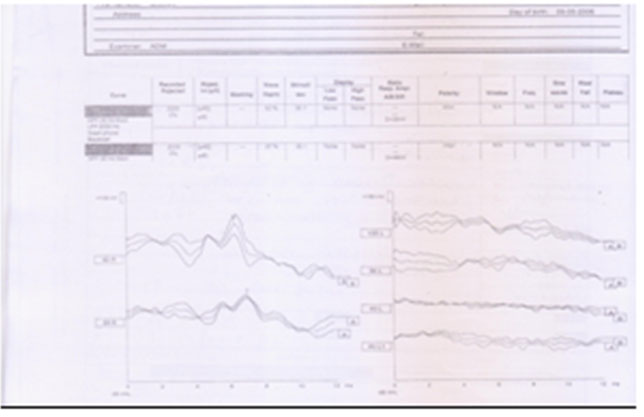
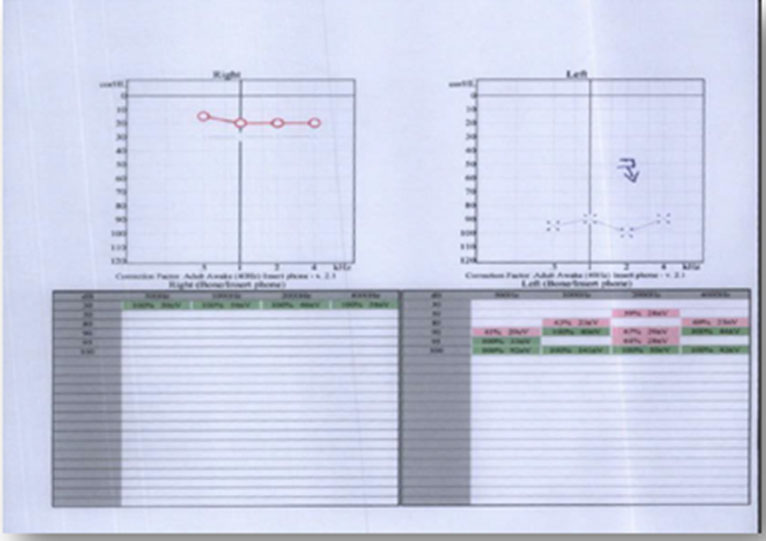
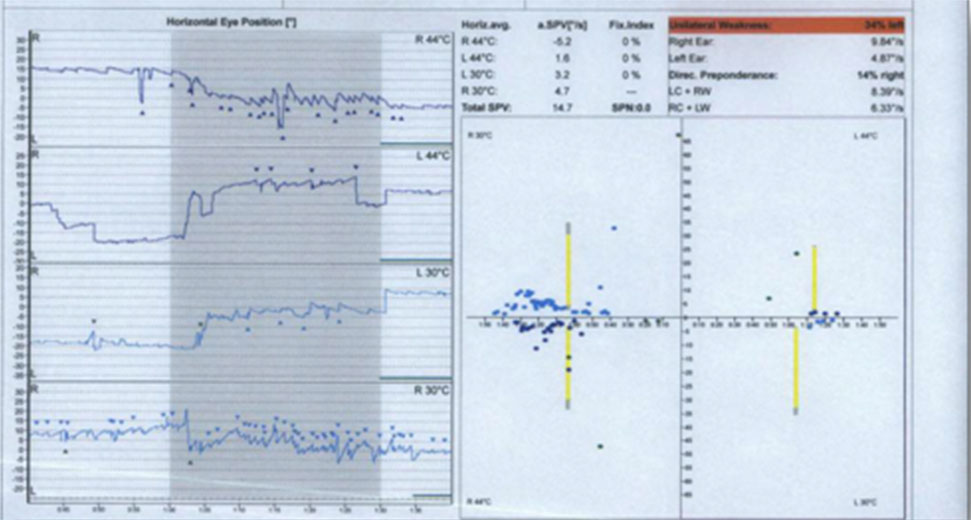
A 13-year-old female patient presented to Otorhinolaryngology Head & Neck Surgery (ORL H&NS) clinic at Prince Sultan Military Medical City with a history of difficulty in hearing in the left ear with unknown exact onset. Her father reported that they had been informed by the school teacher that the child did not pass the school’s hearing test on the left ear. The child denied other associated symptoms such as tinnitus and vertigo. No history of previous ear diseases or serious childhood infections. Pre-, peri-, and postnatal history was unremarkable. Past medical, surgical history, and family history were irrelevant. Ear-nose-throat (ENT) examination was without abnormalities. Otoscopic inspection revealed normal eardrums. Cranial nerves evaluation revealed no neurological deficit apart from difficulties in hearing in the left side. Weber’s test localized to the right ear. No observed spontaneous or induced nystagmus. Audiological evaluation disclosed the following: tympanogram showed bilateral type A graph, suggestive of normal middle ear function (Figure 1). Puretone audiometry (PTA) demonstrated normal hearing in the right side and left-sided profound sensorineural hearing loss (Figure 2). Auditory brainstem responses (ABR) and auditory steady-state response (ASSR) confirmed PTA results (Figure 3 and Figure 4). Caloric testing revealed left canal paresis of 34% (Figure 5). The results of the caloric test, in provisions of the responses to four air stimuli, were used to attain measures of horizontal canal status. Comprehensive laboratory investigations that included a hormonal panel, biochemistry, and viral serology were unremarkable for underlying pathology. Routine non-enhanced MR sequences were obtained (T1, T2, DWI, FIESTA, and T1 post-contrast and with fat suppression). The MRI revealed that there is a left-sided neural vascular conflict of the AICA loop (Figure 6), which is abutting the cisternal segment of the cochlear nerve proximal to the entrance of the internal auditory canal. The conflict corresponds to faint abnormal enhancement perceived in both axial and coronal acquisitions. Both inner ear structures were within normal limits in terms of formation and signal intensity. There was no diffusion restriction. The brain showed normal gray-white matter differentiation, normal ventricles, and CSF spaces. Magnetic resonance imaging findings were suggestive of neural-vascular conflict between the AICA loop and the left cochlear nerve. On that basis, single-sided deafness related to NVC between the AICA loop and the left cochlear nerve was diagnosed.
Microvascular decompression (MVD) of the vestibulocochlear nerve is possibly helpful in special cases that reveal pulsatile tinnitus or unbearable positional vertigo. Unfortunately, there is no supporting evidence until this time for the efficacy of MVD for SNHL.
Parents conveyed their distress of their child being rejected or bullied because of the stigma of SSD or wearing hearing aids. This distress leads parents to decide against the usage of hearing aids. Parents and patient were counseled that single-sided deafness cannot be cured. Nevertheless, there is more than one option to lessen the difficulties in hearing from that side. These options are: cochlear implantation (CI) and varying types of hearing aids such as contralateral routing of sound systems (CROSS) hearing aids or bone conduction devices (BCD). This is achieved by transmitting sound from the deaf side to the hearing ear. In addition, the patient was educated on listening strategies and coping through considering the best setting and listening location besides reducing background noise whenever possible, all of this should be with reasonable expectations.



Discussion
This case report demonstrated an uncommon pathology for SSD, which was found in a 13-year-old girl, and as mentioned in the previous studies, NVC is a recognized cause for SSD. There is considerable controversy in the literature regarding the effect of AICA on the VIIIth cranial nerve with a hearing loss sequelae [12]. Contrarily, individuals may have no symptoms in spite of positive MRI findings [13].
This young girl and her family were facing personal challenges in regard to her hearing difficulty. The psychosocial consequences of dealing with the burden of the illness itself and the dispreference of using a hearing aid, which rooted from the fear of social stigma, were other hurdles to be considered. The role of audiological assessment and follow-up is crucial, not only for clinical diagnosis, but for a rather comprehensive approach that includes the patient and the family’s biopsychosocial needs.
The first step in the audiological evaluation was following the usual model of history taking and audiological evaluation with PTA, ABR, and ASSR. These tests confirmed the profound sensory hearing loss of the left ear and assessed the function of the right ear to be normal without any hearing loss. Hence, ordering an MRI was essential. Moreover, the MRI that was requested to look for an underlying cause found that the NVC was also on the left side only, and this correlates to the area of the patient’s pathology.
Evaluation of patients with SSD is an important measure for appropriate management. Magnetic resonance imaging is an important diagnostic tool that also helps in informed therapy planning, and it is the responsibility of the physician to evaluate the outcome of investigations, the need for further action, and a befitting referral where necessary. In this case, SSD was linked to NVC on the basis of MRI finding and in view of the fact that clinical history and other investigations did not justify another cause.
Etiological evaluation is a crucial step toward better management with an effective counseling process for patients and parents. Magnetic resonance imaging is an important diagnostic tool that also helps in informed therapy planning [14]. Unfortunately, up until now, there is no supporting evidence for the efficacy of MVD of the vestibulocochlear nerve for SNHL. Microvascular decompression of the vestibulocochlear nerve is possibly helpful in special cases with tinnitus or unbearable vertigo linked to vascular compression [15].
Single-sided deafness is usually managed with BCD and CROSS. This results in a fair enhancement of subjective speech conversation. The BCD and CROSS do not help in sound localization. Both devices lead to the same sound localization ability compared to the unaided condition. Unfortunately, the supporting evidence for these devices to improve understanding speech in noise or localization of sound is limited [16]. Regrettably, they also have a small-to-medium impact on health-related quality of life (HRQoL), speech, spatial, and qualities of hearing scale health utility index mark 3 (HUI3) [17]. To support any future recommendations for the clinical management of SSD, there is a great need for prospective controlled studies that quantify consequences with restriction of biases [18]. The CI is a superior management option over BCD and CROSS devices. It permits binaural hearing and the ability to localize sound together with a better understanding of speech in a noisy situation [3]. Early CI with congenital SSD will result in remarkable outcomes, delay in implantation will limit benefit. In post-lingual SSD, the earlier the child is implanted, the better the outcome [19].
Conclusion
In conclusion, this report described an uncommon pathology for SSD. The causes of SSD may be overlooked when investigations apart from MRI are normal. However, this should not exhaust physicians to look for an underlying cause whenever MRI is available, as in this case, where NVC was the most likely reason for SSD. Having a diagnosis can help the parents and the patient in finding closure for the reason for their illness and move on with the management. Provided with the evidence, this will aid in patient education, counseling, and tailoring the management plan according to the individual needs of the patients and their families. Additional cost-effective studies on the best management for SSD and exploring psychological and social consequences must be carried out, to assure a high standard of delivered care. Evidence-based decision-making empowers professionals to face challenges in convincing the child and parents to offer interventions that tremendously improve the child’s outcomes and outweigh any stigma.
REFERENCES
1.
Dwyer NY, Firszt JB, Reeder RM. Effects of unilateral input and mode of hearing in the better ear: Self-reported performance using the speech, spatial and qualities of hearing scale. Ear Hear 2014;35(1):126–36. [CrossRef]
[Pubmed]

2.
Kwak C, Kim S, Lee J, Seo Y, Kong T, Han W. Speech perception and gap detection performance of single-sided deafness under noisy conditions. J Audiol Otol 2019;23(4):197–203. [CrossRef]
[Pubmed]
3.
Liu J, Zhou M, He X, Wang N. Single-sided deafness and unilateral auditory deprivation in children: Current challenge of improving sound localization ability. J Int Med Res 2020;48(1):300060519896912. [CrossRef]
[Pubmed]
4.
Li X, Qiao Y, Shen H, Niu Z, Shang Y, Guo H. Topological reorganization after partial auditory deprivation—a structural connectivity study in single-sided deafness. Hear Res 2019;380:75–83. [CrossRef]
[Pubmed]
5.
van Wieringen A, Boudewyns A, Sangen A, Wouters J, Desloovere C. Unilateral congenital hearing loss in children: Challenges and potentials. Hear Res 2019;372:29–41. [CrossRef]
[Pubmed]
6.
Baldauf J, Rosenstengel C, Schroeder HWS. Nerve compression syndromes in the posterior cranial fossa: Diagnosis and treatment. Dtsch Arztebl Int 2019;116(4):54–60. [CrossRef]
[Pubmed]
7.
Bhatoe HS. The neurovascular syndromes: A review of pathophysiology – Lessons learnt from Prof. Chandy’s paper published in 1989. Neurol India 2019;67(2):377–88. [CrossRef]
[Pubmed]
8.
Alonso F, Kassem MW, Iwanaga J, et al. Anterior inferior cerebellar arteries juxtaposed with the internal acoustic meatus and their relationship to the cranial nerve VII/VIII complex. Cureus 2017;9(8):e1570. [CrossRef]
[Pubmed]
9.
van Beeck Calkoen EA, Engel MSD, van de Kamp JM, et al. The etiological evaluation of sensorineural hearing loss in children. Eur J Pediatr 2019;178(8):1195–205. [CrossRef]
[Pubmed]
10.
Chadha NK, Weiner GM. Vascular loops causing otological symptoms: A systematic review and meta-analysis. Clin Otolaryngol 2008;33(1):5–11. [CrossRef]
[Pubmed]
11.
Roldán-Fidalgo A, Rodríguez-Valiente A, González FM, Pinilla M, Trinidad A, Álvarez BB. Vascular loops and neuro-otologic symptoms: Is there any correlation. IJOHNS 2013;2(6):245–7. [CrossRef]
12.
Moosa S, Fezeu F, Kesser BW, Ramesh A, Sheehan JP. Sudden unilateral hearing loss and vascular loop in the internal auditory canal: Case report and review of literature. J Radiosurg SBRT 2015;3(3):247–55.
[Pubmed]
13.
Oztek MA, Çakar I, Karaali K, Senol U. Evaluation of AICA and vestibulocochlear nerve relationship in patients with vertigo. European Society of Radiology 2017. [CrossRef]
14.
Lipschitz N, Kohlberg GD, Scott M, Greinwald JH Jr. Imaging findings in pediatric single-sided deafness and asymmetric hearing loss. Laryngoscope 2020;130(4):1007–10. [CrossRef]
[Pubmed]
15.
Turcotte EL, Patra DP, Abi-Aad KR, Welz ME, Weisskopf PA, Bendok BR. Microvascular decompression and transposition of the 8th cranial nerve using a fenestrated clip. World Neurosurg 2020;135:233. [CrossRef]
[Pubmed]
16.
Peters JPM, Smit AL, Stegeman I, Grolman W. Review: Bone conduction devices and contralateral routing of sound systems in single-sided deafness. Laryngoscope 2015;125(1):218–26. [CrossRef]
[Pubmed]
17.
Kitterick PT, Lucas L, Smith SN. Improving healthrelated quality of life in single-sided deafness: A systematic review and meta-analysis. Audiol Neurootol 2015;20 Suppl 1:79–86. [CrossRef]
[Pubmed]
18.
Kitterick PT, Smith SN, Lucas L. Hearing instruments for unilateral severe-to-profound sensorineural hearing loss in adults: A systematic review and meta-analysis. Ear Hear 2016;37(5):495–507. [CrossRef]
[Pubmed]
19.
Ramos Macías Á, Borkoski-Barreiro SA, Falcón González JC, de Miguel Martínez I, Ramos de Miguel Á. Single-sided deafness and cochlear implantation in congenital and acquired hearing loss in children. Clin Otolaryngol 2019;44(2):138–43. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Mona S Al Rakaf - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2020 Mona S Al Rakaf. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}