 |
Case Report
Highlights of serious distant effects after local injection of botulinum toxin therapy: A report of pediatric case
1 Assistant Professor of Clinical Toxicology-Poison Control Center, Department of Forensic Medicine & Clinical Toxicology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Address correspondence to:
Hoda M Salah Eldin
Department of Forensic Medicine & Clinical Toxicology, Faculty of Medicine, Ain Shams University, Cairo,
Egypt
Message to Corresponding Author
Article ID: 101127Z01EM2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Mohammed EA, Salah Eldin HM. Highlights of serious distant effects after local injection of botulinum toxin therapy: A report of pediatric case. Int J Case Rep Images 2020;11:101127Z01EM2020.ABSTRACT
Introduction: Botulinum neurotoxin A (BoNT-A) is widely used in various conditions that cause involuntary muscle contractions, such as management of spasticity in cerebral palsy (CP). However, iatrogenic botulism resulting from systemic effects from BoNT-A is uncommon but may have serious life-threatening consequences.
Case Report: We report a case of pediatric patient who developed iatrogenic botulism after therapeutic intramuscular injections of BoNT-A.
Conclusion: This case highlights the importance of clinicians having adequate information of the risk of systemic botulism following local injections of BoNT-A and caution is needed in using this therapy.
Keywords: Botulinum neurotoxin A, Iatrogenic botulism
Introduction
Botulism is a rare, paralytic illness produced by neurotoxin of Clostridium botulinum, an anaerobic, spore-forming bacterium [1]. Botulism, if left untreated, may cause respiratory failure and even death [2]. Three botulinum neurotoxins (A, B, and E) out of nine types (BoNT, serotypes A–H) are most commonly responsible for human diseases [3],[4].
Botulinum neurotoxins when injected locally into the muscle act at the neuromuscular junction resulting in dose-dependent muscle paralysis [3]. Clinically, it causes reversible muscle weakness and inhibits acetylcholine release for about three months [5].
Botulinum toxin type A is widely used for treatment of various disorders, such as spasticity, dystonia, hyperhidrosis, sialorrhea, and neurogenic bladder. In addition, BoNT-A has been used for prophylaxis of chronic migraine, as well as for cosmetic purposes [6]. Although BoNT-A therapy has been generally reported as safe, it can cause postinjection rare but serious adverse events [7]. Cases of iatrogenic botulism, a potentially fatal subtype of botulism, have been infrequently described [8],[9],[10],[11],[12],[13],[14]. Details of the adverse effects and deaths following treatment with BoNT-A in children with CP are limited. However, four deaths of children with cerebral palsy in the United States and one in Europe have been reported [14],[15]. In this study, we describe a case of a child with CP who developed iatrogenic botulism after injections of therapeutic doses of botulinum toxin for lower limb spasticity.
Case Report
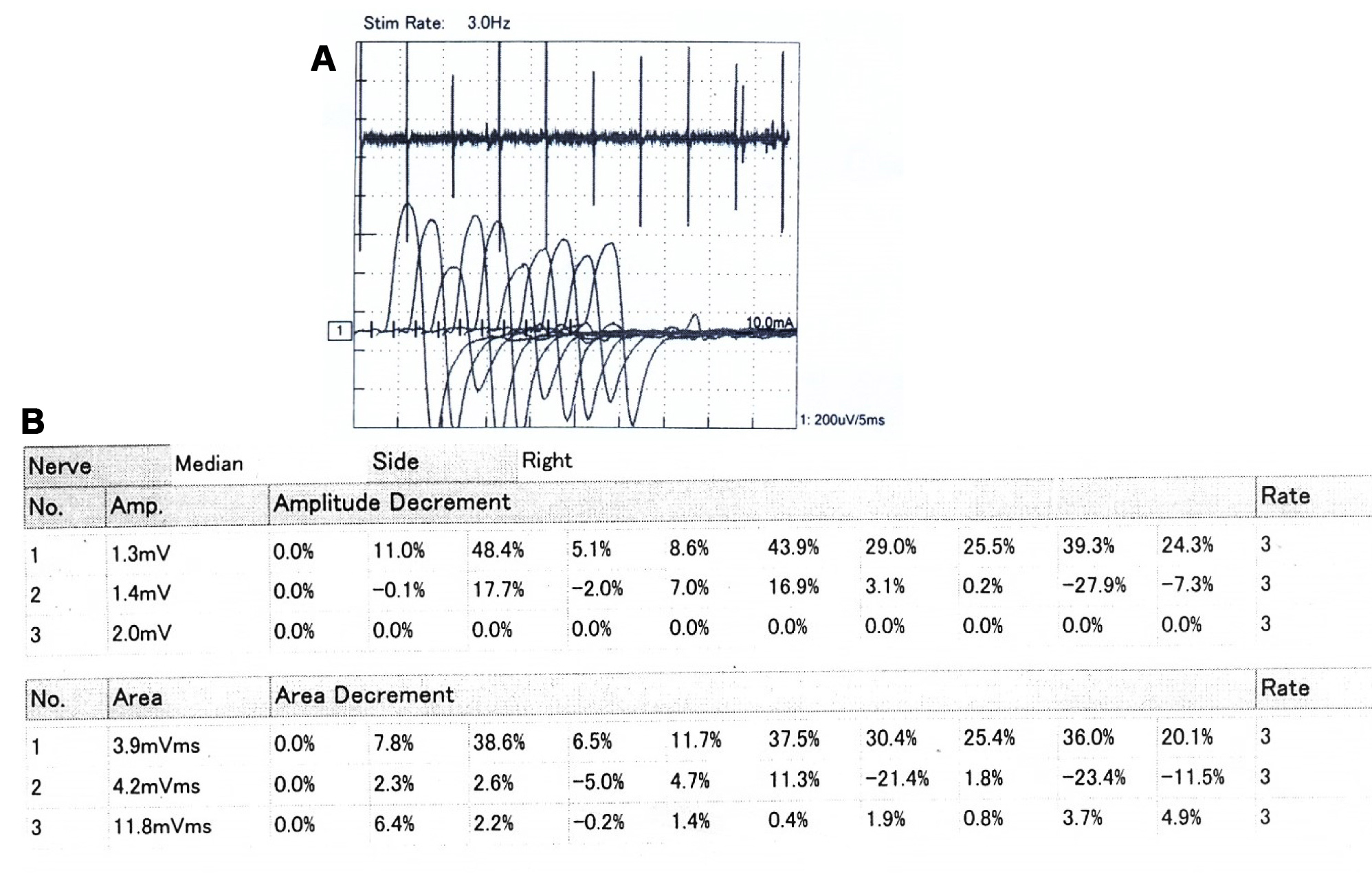
A 5-year-old male child with CP presented with botulism-like manifestations 10 days after receiving multilevel injections, total dose of 500 units of BoNT-A (Dysport®) in his lower limbs to relieve muscle spasticity. Manifestations begun three days after the injections, his mother started to notice drooling then swallowing The patient condition dramatically improved after completion of first dose, a second dose was given 12 hours later (total dose of 1 vial) after which mild additional improvement was noted. Ptosis and muscle weakness greatly improved while dysphagia and constipation only mildly improved. The patient was discharged after eight days of hospitalization, but he was readmitted four days later because of persistent dysphagia to solid and constipation. Another third dose of botulism antitoxin was given, and Ryle feeding was started. Motor nerve conduction study of right median and common peroneal nerves showed average motor latency and conduction velocity of both tested nerves with average wave forms of compound muscle action potential compound muscle action potential (CMAP; Figure 1). Repetitive nerve stimulation (RNS) was done to assess the neuromuscular junction state. It had irregular results varying between average and mild incremental responses especially of right median nerve indicating a partial effect on neuromuscular junction (Figure 2). On the next day of readmission gag reflex was good, thus, oral feeding was encouraged, and he was discharged two days later. Finally, the symptoms were gradually resolved on subsequent follow-up visits and completely recovered in two months.

Discussion
There are several forms of botulism including foodborne, aerosolized, infantile, wound, iatrogenic, and intestinal botulism [16]. Botulism is a potentially fatal illness, regardless of exposure mechanism. Early diagnosis of botulism, appropriate treatment in an intensive care unit, supply of mechanical ventilation if needed, and administration of botulism antitoxin have been associated with favorable outcome [17],[18].
The most potent serotype of botulinum toxins is BoNT-A, its toxicity is one million-fold higher than toxin of cobra [19]. The mechanism of action of BoNT-A is acetylcholine release inhibition at the neuromuscular junction, resulting in chemical denervation and paralysis of muscle [20].
Botulinum toxin A use has become expanding worldwide which raises safety issue, one of commonly used indication of BoNT-A therapy is the treatment of dystonia and spasticity in children with CP [21]. In spite of well-established experience on efficacy and safety, awareness about postinjection serious adverse effects of the botulinum toxin is essential. Botulinum toxin A safety has been questioned after serious adverse event reports following its use like dysphagia, generalized paralysis, respiratory depression, and even death [9]. A study by Phadke et al. [20] reported the adverse effects of BoNT-A injections for spasticity in Canada. Of all adverse events reported, 8% were deaths. It is difficult to assess the incidence of serious adverse effects due to underreporting worldwide, however, case reports and case series are a cornerstone of drug safety research [22].
In our patient, the diagnosis of iatrogenic botulism is based on history of recent BoNT-A intramuscular injections and clinical course and findings (bilateral ptosis, dysphagia, and generalized weakness) consistent with botulism.
Onset of symptoms may occur within an incubation period of botulism range from 6 hours to 10 days [21]. Clinical signs and symptoms of botulism awareness is essential for early diagnosis, while waiting for laboratory or electrophysiological confirmation is a fault [23]. However, diagnosis in sporadic cases is usually missed because botulism is a rare disease.
There are no definite recommendations on an optimal injection doses for BoNT-A for adults or children. The commonly used two formulations of BoNT-A are Botox and Dysport. Studies in adults report that 1 U of Botox is equivalent to 3 U of Dysport, but in children there have been no studies investigating equivalent doses of these two formulations [21].
Published studies confirm that there has been a massive variation in doses of BoNT-A administered in single treatment session in children with spastic cerebral palsy over the last 15 years [24],[25],[26],[27],[28]. Additionally, there is variation in number of muscles injected, dilution, and whether BoNT-A toxin should be given based on fat-free mass or body weight [21]. In multilevel injection protocols, the increase in total dose mainly due to increasing numbers of muscles injected during one session [28],[29]].
Wissel et al. [1] found a greater improvement in spasticity with a higher dose of Botox. Polak et al. [30] also concluded greater efficacy with higher doses using Dysport and found that the optimal total dose of Dysport formulation would be between 200 and 500 U.
Naidu et al. [31] found higher BoNT-A doses to be associated with increased risk of systemic and respiratory complications. Coté et al. [7] reported that serious adverse effects of botulinum toxin A, as iatrogenic botulism, are commonly seen with higher doses associated with therapeutic use, and incidence is less commonly reported with cosmetic use. However, Fan et al. [9] disagreed and reported two cases of iatrogenic botulism following cosmetic use and suggested that deviation from recommended indication, improper injection, and mishandling of the drug may be more in cosmetic use.
In 2008, Public Citizen requested the agency of US Federal Drug Administration to increase its warning on the labels of commercial products of BoNT-A toxin [32]. Although the precise human lethal dose of botulinum toxin A is not known, extrapolation from animal studies suggests an approximate human lethal dose of 40 U/kg [2].
An alarming question is how we could prevent the possible adverse events of botulinum toxin. Clinicians administering botulinum toxin should have sufficient knowledge about anatomy of muscles involved and accurate selection of injection sites and applying the correct dose with proper process of dilution, storage, and handling of the product [10]. The agent of choice for drug dilution is saline, some errors in injection and storage include injecting the product after the 4-hour expiration time, freezing the product for future use, and using a vial of botulinum toxin-A for many patients [7].
Diffusion of botulinum toxin in the injected muscle and adjacent muscles has been most commonly reported even diffusion of botulinum toxin to contralateral muscles has also been documented resulting in acute muscle paresis. Muscle weakness attributed to high dose of toxin injected [33].
Generalized weakness of muscles remote to injection sites is much less common yet reported as an adverse effect in some studies [34]. Systemic adverse effects occur in 1–2% of children with CP following BoNT-A toxin injection [31]. Systemic toxin spread can lead to adverse effects of botulism, including muscle paralysis, dysphonia, dysarthria, dysphagia, respiratory depression, and even death. The mechanism responsible for generalized diffusion of botulinum toxin is not well known. Possible explanation includes either a systemic spread by blood circulation or a retrograde axonal transport of toxin [35].
Vascular spread is possible through means other than direct administration into the blood circulation because needles are aspirated for blood before injections. It is possible that vascular spread occurs via absorption through the capillary bed [20].
Based on experimental studies, Wiegand et al. [36] reported retrograde axonal transport of radioactive BoNT-A toxin the corresponding via spinal cord segments. More recent studies showed retrograde transport of active toxin molecules through microtubules in the axon to both motor and sensory regions in the spinal cord after intramuscular and intraneural injections of BoNT-A [37],[38]. In addition, experimental study by Curra and Berardelli [39] found that botulinum toxin receptors exist in the central nervous system and small amount of toxin crosses the blood-brain barrier. This raises the possibility of retrograde transport of botulinum toxin is similar to tetanus toxin, and may result in centrally mediated adverse effects.
Prolonged latency in occurrence of adverse events is not a characteristic of vascular toxin spread. Retrograde transport in such cases appears more likely. However, it is possible that a combination of both vascular and retrograde axonal spread of toxin is responsible for remote adverse effects [40].
Electrophysiological studies represent a useful tool to confirm the diagnosis of iatrogenic botulism. However, there is no highly specific findings of electrodiagnostic abnormalities in iatrogenic botulism and clinico-electrophysiological correlation is necessary to make the diagnosis [41]. Repetitive nerve stimulation in our patient showed mild incremental responses, suggestive of partial effect of BoNT-A injections on neuromuscular junction.
The diagnosis of iatrogenic botulism is based on history of recent BoNT-A injections and clinical findings. Waiting for electrophysiological or laboratory confirmation is an error, while clinician awareness of signs and symptoms of botulism is essential for early diagnosis [23]. In our patient, the clinical course and EMG findings were compatible with a neuromuscular junction disorder suggestive of iatrogenic botulism because of therapeutic use of Dysport.
Botulism is a potentially severe lethal paralytic illness, regardless of exposure source. Early management in an intensive care unit, administration of botulinum antitoxin, and applying mechanical ventilation when indicated have been associated with better outcome [2]. Apart from supportive management, botulinum antitoxin is the mainstay of therapy. Antitoxin acts by neutralizing unbound botulinum toxin, the duration of antitoxin efficiency is unknown. In a case series, rapid recovery occurred for patients with wound botulinum who were managed with botulinum antitoxin four days of symptom onset [17]. However, in an outbreak of foodborne botulism detection of toxin in the blood of a patient up to 25 days after symptom onset was demonstrated [42].
In general, data on iatrogenic botulism is limited and the efficacy of antitoxin therapy is controversial. In a case report, a woman with botulism induced by cosmetic BoNT-A injection showed no improvement following antitoxin administration six days after symptom onset [43]. By contrast, clinical response was observed in two female patients to whom antitoxin therapy for iatrogenic botulism after cosmetic injection of BoNT-A was delayed to the seventh and ninth days after symptom onset [9]. In our patient, antitoxin was administered 10 days after symptom onset. Despite the delay in antitoxin therapy, most patients’ symptoms showed dramatic improvement except for dysphagia and constipation only mildly improved and gradually reversed during the following weeks.
Clinical improvement after antitoxin treatment might be because of neutralization of persistent circulating toxin in the bloodstream, and which may be contributive if their neuromuscular junction receptors are not fully saturated by the BoNT-A. In addition, it is likely that there was BoNT-A redistribution from its receptors before the step of irreversible endocytosis occurs [44]. Moreover, botulinum antitoxin therapy has been shown to accelerate neuromuscular conduction by increasing acetylcholine release from autonomic cholinergic nerve terminals [45].
Conclusion
Systemic features of iatrogenic botulism are infrequent but may lead to life-threatening events. Diagnosis is based on both history of recent injection of BoNT toxin and clinical manifestations. Clinician and patients need to be aware of the possible risks associated with injection of botulinum toxin. Clinical response of the patient in this report and other studies in literature suggest that administration of antitoxin should be considered even if the case present late. Serious adverse effects from approved medications should be reported to prevent future unfavorable outcomes.
REFERENCES
1.
Wissel J, Heinen F, Schenkel A, et al. Botulinum toxin A in the management of spastic gait disorders in children and young adults with cerebral palsy: A randomized, double-blind study of “high-dose” versus “low-dose” treatment. Neuropediatrics 1999;30(3):120–4. [CrossRef]
[Pubmed]

2.
Chertow DS, Tan ET, Maslanka SE, et al. Botulism in 4 adults following cosmetic injections with an unlicensed, highly concentrated botulinum preparation. JAMA 2006;296(20):2476–9. [CrossRef]
[Pubmed]
3.
Rossetto O, Pirazzini M, Montecucco C. Botulinum neurotoxins: Genetic, structural and mechanistic insights. Nat Rev Microbiol 2014;12(8):535–49. [CrossRef]
[Pubmed]
4.
Dover N, Barash JR, Hill KK, Xie G, Arnon SS. Molecular characterization of a novel botulinum neurotoxin type H gene. J Infect Dis 2014;209(2):192–202. [CrossRef]
[Pubmed]
5.
Howell K, Selber P, Graham HK, Reddihough D. Botulinum neurotoxin A: An unusual systemic effect. J Paediatr Child Health 2007;43(6):499–501. [CrossRef]
[Pubmed]
6.
Pirazzini M, Rossetto O, Eleopra R, Montecucco C. Botulinum neurotoxins: Biology, pharmacology, and toxicology. Pharmacol Rev 2017;69(2):200–35. [CrossRef]
[Pubmed]
7.
Coté TR, Mohan AK, Polder JA, Walton MK, Braun MM. Botulinum toxin type A injections: Adverse events reported to the US Food and Drug Administration in therapeutic and cosmetic cases. J Am Acad Dermatol 2005;53(3):407–15. [CrossRef]
[Pubmed]
8.
Szuch E, Caress JB, Paudyal B, Brashear A, Cartwright MS, Strowd RE 3rd. Head drop after botox: Electrodiagnostic evaluation of iatrogenic botulinum toxicity. Clin Neurol Neurosurg 2017;156:1–3. [CrossRef]
[Pubmed]
9.
Fan KL, Wang YL, Chu G, Leung LP. Delayed antitoxin treatment of two adult patients with botulism after cosmetic injection of botulinum type A toxin. J Emerg Med 2016;51(6):677–9. [CrossRef]
[Pubmed]
10.
Ghasemi M, Norouzi R, Salari M, Asadi B. Iatrogenic botulism after the therapeutic use of botulinum toxin-A: A case report and review of the literature. Clin Neuropharmacol 2012;35(5):254–7. [CrossRef]
[Pubmed]
11.
Coban A, Matur Z, Hanagasi HA, Parman Y. Iatrogenic botulism after botulinum toxin type A injections. Clin Neuropharmacol 2010;33(3):158–60. [CrossRef]
[Pubmed]
12.
Crowner BE, Torres-Russotto D, Carter AR, Racette BA. Systemic weakness after therapeutic injections of botulinum toxin A: A case series and review of the literature. Clin Neuropharmacol 2010;33(5):243–7. [CrossRef]
[Pubmed]
13.
Varghese-Kroll E, Elovic EP. Contralateral weakness and fatigue after high-dose botulinum toxin injection for management of poststroke spasticity. Am J Phys Med Rehabil 2009;88(6):495–9. [CrossRef]
[Pubmed]
14.
Davy M, Robinson K, Taylor E. Botulinum toxin type A (Botox) and distal toxin spread. Can Adv React Newsl 2008;18:1.
15.
Topliss D, Goed M, Kotsisilos V, et al. Adverse reactions with botulinum toxin A (Botox, Dysport). Aust Adv Drug Reactions Bull 2009;28:2.
16.
Rashid EAMA, El-Mahdy NM, Kharoub HS, Gouda AS, ElNabarawy NA, Mégarbane B. Iatrogenic botulism outbreak in Egypt due to a counterfeit botulinum toxin A preparation – A descriptive series of patient features and outcome. Basic Clin Pharmacol Toxicol 2018;123(5):622–7. [CrossRef]
[Pubmed]
17.
Chang GY, Ganguly G. Early antitoxin treatment in wound botulism results in better outcome. Eur Neurol 2003;49(3):151-3. [CrossRef]
[Pubmed]
18.
Sandrock CE, Murin S. Clinical predictors of respiratory failure and long-term outcome in black tar heroin-associated wound botulism. Chest 2001;120(2):562–6. [CrossRef]
[Pubmed]
19.
Shaw L, Rodgers H, Price C, et al. BoTULS: A multicentre randomised controlled trial to evaluate the clinical effectiveness and cost-effectiveness of treating upper limb spasticity due to stroke with botulinum toxin type A. Health Technol Assess 2010;14(26):1–113, ii–iv. [CrossRef]
[Pubmed]
20.
Phadke CP, Balasubramanian CK, Holz A, Davidson C, Ismail F, Boulias C. Adverse clinical effects of botulinum toxin intramuscular injections for spasticity. Can J Neurol Sci 2016;43(2):298–310. [CrossRef]
[Pubmed]
21.
Crowner BE, Brunstrom JE, Racette BA. Iatrogenic botulism due to therapeutic botulinum toxin a injection in a pediatric patient. Clin Neuropharmacol 2007;30(5):310–3. [CrossRef]
[Pubmed]
22.
Abou Chakra CN, Pariente A, Pinet M, Nkeng L, Moore N, Moride Y. Case series in drug safety: A review to determine characteristics and quality. Drug Saf 2010;33(12):1081–8. [CrossRef]
[Pubmed]
23.
Zhang JC, Sun L, Nie QH. Botulism, where are we now? Clin Toxicol (Phila) 2010;48(9):867–9. [CrossRef]
[Pubmed]
24.
Corry IS, Cosgrove AP, Duffy CM, McNeill S, Taylor TC, Graham HK. Botulinum toxin A compared with stretching casts in the treatment of spastic equinus: A randomised prospective trial. J Pediatr Orthop 1998;18(3):304–11.
[Pubmed]
25.
Desloovere K, Molenaers G, Jonkers I, et al. A randomized study of combined botulinum toxin type A and casting in the ambulant child with cerebral palsy using objective outcome measures. Eur J Neurol 2001;8 Suppl 5:75–87. [CrossRef]
[Pubmed]
26.
Graham HK, Aoki KR, Autti-Rämö I, et al. Recommendations for the use of botulinum toxin type A in the management of cerebral palsy. Gait Posture 2000;11(1):67–79. [CrossRef]
[Pubmed]
27.
Koman LA, Mooney JF 3rd, Smith BP, Goodman A, Mulvaney T. Management of spasticity in cerebral palsy with botulinum-A toxin: Report of a preliminary, randomized, double-blind trial. J Pediatr Orthop 1994;14(3):299–303. [CrossRef]
[Pubmed]
28.
Molenaers G, Desloovere K, De Cat J, et al. Single event multilevel botulinum toxin type A treatment and surgery: similarities and differences. Eur J Neurol 2001;8 Suppl 5:88–97. [CrossRef]
[Pubmed]
29.
Heinen F, Molenaers G, Fairhurst C, et al. European consensus table 2006 on botulinum toxin for children with cerebral palsy. Eur J Paediatr Neurol 2006;10(5–6):215–25. [CrossRef]
[Pubmed]
30.
Polak F, Morton R, Ward C, Wallace WA, Doderlein L, Siebel A. Double-blind comparison study of two doses of botulinum toxin A injected into calf muscles in children with hemiplegic cerebral palsy. Dev Med Child Neurol 2002;44(8):551–5. [CrossRef]
[Pubmed]
31.
Naidu K, Smith K, Sheedy M, Adair B, Yu X, Graham HK. Systemic adverse events following botulinum toxin A therapy in children with cerebral palsy. Dev Med Child Neurol 2010;52(2):139–44. [CrossRef]
[Pubmed]
32.
Public Citizen’s Health research Group. Petition requesting regulatory action concerning the spread of botulinum toxin (Botox, Myobloc) to the other parts of the body. 2008. [Available at: http://www.citizen.org/article/petition-requesting-regulatory-action-concerning-the-spread-of-botulinum-toxin-botox-myobloc-to-other-parts-of-the-body]
33.
Yaraskavitch M, Leonard T, Herzog W. Botox produces functional weakness in non-injected muscles adjacent to the target muscle. J Biomech 2008;41(4):897–902. [CrossRef]
[Pubmed]
34.
Bakheit AM, Ward CD, McLellan DL. Generalised botulism-like syndrome after intramuscular injections of botulinum toxin type A: A report of two cases. J Neurol Neurosurg Psychiatry 1997;62(2):198. [CrossRef]
[Pubmed]
35.
Yiannakopoulou E. Serious and long-term adverse events associated with the therapeutic and cosmetic use of botulinum toxin. Pharmacology 2015;95(1–2):65–9. [CrossRef]
[Pubmed]
36.
Wiegand H, Erdmann G, Wellhöner HH. 125I-labelled botulinum A neurotoxin: Pharmacokinetics in cats after intramuscular injection. Naunyn Schmiedebergs Arch Pharmacol 1976;292(2):161–5. [CrossRef]
[Pubmed]
37.
Matak I, Bach-Rojecky L, Filipović B, Lacković Z. Behavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin A. Neuroscience 2011;186:201–7.
38.
Matak I, Riederer P, Lacković Z. Botulinum toxin’s axonal transport from periphery to the spinal cord. Neurochem Int 2012;61(2):236–9. [CrossRef]
[Pubmed]
39.
Currà A, Berardelli A. Do the unintended actions of botulinum toxin at distant sites have clinical implications? Neurology 2009;72(12):1095–9. [CrossRef]
[Pubmed]
40.
Papadonikolakis AS, Vekris MD, Kostas JP, Korompilias AV, Soucacos PN. Transient erectile dysfunction associated with intramuscular injection of botulinum toxin type A. J South Orthop Assoc 2002;11(2):116–8.
[Pubmed]
41.
Leonardi L, Haggiag S, Petrucci A, Lispi L. Electrophysiological abnormalities in iatrogenic botulism: Two case reports and review of the literature. J Clin Neurosci 2019;60:138–41. [CrossRef]
[Pubmed]
42.
Sheth AN, Wiersma P, Atrubin D, et al. International outbreak of severe botulism with prolonged toxemia caused by commercial carrot juice. Clin Infect Dis 2008;47(10):1245–51. [CrossRef]
[Pubmed]
43.
Souayah N, Karim H, Kamin SS, McArdle J, Marcus S. Severe botulism after focal injection of botulinum toxin. Neurology 2006;67(10):1855–6. [CrossRef]
[Pubmed]
44.
Rossetto O, Pirazzini M, Montecucco C. Botulinum neurotoxins: Genetic, structural and mechanistic insights. Nat Rev Microbiol 2014;12(8):535–49. [CrossRef]
[Pubmed]
45.
Cheringcon M. Clinical spectrum of botulism. Muscle Nerve 1998;21(6):701–10. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Eman Abdelfatah Mohammed - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hoda M Salah Eldin - Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Eman Abdelfatah Mohammed et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}