 |
Clinical Image
Sudden onset of vomiting and intestinal ischemia during the treatment of chronic atrial fibrillation
1 Department of General Medicine, Akiota Hospital, Hiroshima, Japan
Address correspondence to:
Yasuyuki Taooka
MD, FACP, Department of General Medicine, Akiota Hospital, 236 Shimodomo-Gohchi, Akiota-Cho, Yamagata-Gun, Hiroshima 731-3622,
Japan
Message to Corresponding Author
Article ID: 101111Z01YT2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Taooka Y. Sudden onset of vomiting and intestinal ischemia during the treatment of chronic atrial fibrillation. Int J Case Rep Images 2020;11:101111Z01YT2020.ABSTRACT
No Abstract
Keywords: Atrial fibrillation, Superior mesenteric vein, Thrombosis
Case Report
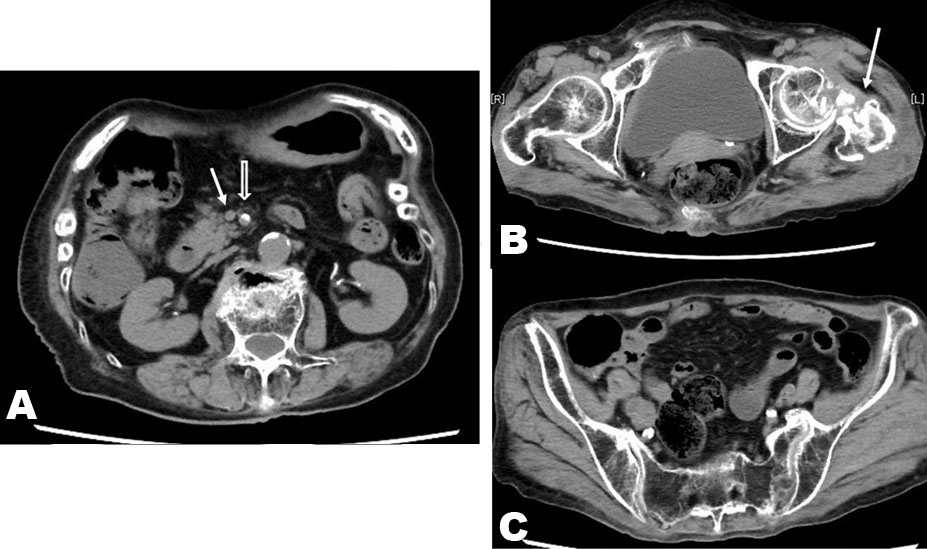
An 86-year-old female during the treatment of atrial fibrillation (AF) consulted our outpatient clinic complained of vomiting for a few hours. She had been administrated with Dabigatran etexilate for nine months as anticoagulant therapy. One day before, she fell down at home in the morning. After that, she noticed left hip pain and had no appetite. On the consult day, she had no abdominal pain and vomiting. Her body temperature was 36.9 °C, and level of her consciousness was clear. Blood pressure was 98/60 mmHg and heart rate was 104/min with irregular rhythm. And there were no other abnormal findings with physical examination. Blood laboratory examination showed as following: white blood cell count 11,920/L, hemoglobin 11.0 g/dL, thrombocyte count 255,000/mL, aspartate aminotransferase (AST) 17 IU/mL, alanine aminotransferase (ALT) 25 IU/mL, lactate dehydrogenase (LDH) 291 U/mL (normal range: 106–211), creatine phosphokinase (CPK) 211 IU/L, blood urea nitrogen (BUN) 31.1 mg/dL, Cr 1.18 mg/dL, brain natriuretic peptide (BNP) 139 pg/mL, C-reactive protein (CRP) 4.87 mg/dL, and blood sugar was 150 mg/dL. Prothrombin time 21.1 seconds (international normalized ratio 2.99), activated partial thromboplastin time 58.1 seconds, and D-dimer was 10.3 g/mL (normal range: 0–0.9). On abdominal computed tomography (CT) (Figure 1), old malunion change of left femur (arrow) was observed (Figure 1B), and mild fluid with gas retention in intentional tract was also shown (Figure 1A and Figure 1B). But there was no evidence of ileus state. Because of renal dysfunction, she could not receive contrast enhanced CT scanning. Considering of her elder age and performance status, intravenous infusion was immediately started with fasting for the treatment of dehydration. And continuous infusion of heparin sodium was also started. Four hours later after admission, suddenly she vomited several times and complained of abdominal pain with right hypochondriac lesion, then the level of her consciousness depressed. Her abdomen was distended and bowel sound was not heard. Atrial blood gas analysis showed metabolic academia as following: pH 7.291, PaCO2 33.1 Torr, PaO2 96.8 Torr, lactate 13.4 mmol/L, and base excess was −10.9 mmol/L. Then abdominal CT scanning was re-examined (Figure 2 and Figure 3). Portal vein gas with left lateral segment of the liver was recognized (Figure 2B), and wall of small intestine was thinned (Figure 2C). Gas was also observed in the mesenteric vein (Figure 3A and Figure 3B). The diameter of superior mesenteric vein (arrow) was smaller than that of superior mesenteric artery (hollow arrow) (Figure 2A). Retrospectively, the diameter of superior mesenteric vein (arrow) of the first abdominal CT imaging was also smaller than that of superior mesenteric artery (hollow arrow) (Figure 1A). From the results of these findings, she had been diagnosed as having wide-range of intestinal ischemia by superior mesenteric artery ischemia. Since general condition was poor and bowel ischemic change was wide-range, there was no surgical indication. Pain control was continued as the conservative treatment, but she passed away on next admission day.


Discussion
Intestinal ischemia including nonocclusive mesenteric ischemia and acute superior mesenteric artery occlusion is known as one of the severe complications of elderly AF [1]. Novel oral anticoagulant, Dabigatran etexilate had been administrated in this case, but thrombosis could not be prevented. As the cause of intestinal ischemia with this case, chronic AF, dehydration, and severe atherosclerotic vascular changes were suspected.
Narrowed diameter of superior mesenteric vein compared with diameter of superior mesenteric artery on CT imaging is known as the sign for ischemia of superior mesenteric artery (smaller superior mesenteric vein sign) [2], [3]. Although the specificity of smaller superior mesenteric vein sign for superior mesenteric artery occlusion is not enough high [3], that findings might become as the early sign of bowel ischemia. Smaller superior mesenteric vein sign is realized to represent decreased blood flow of superior mesenteric artery and reduced venous return [3].
In this case, smaller superior mesenteric vein sign was seen in both CT images of admission and 4 hours later after admission, and blood laboratory data showed hypercoagulability on admission. The possibility of organ ischemia at the point of admission could not be ruled out, and administration of heparin sodium was started. But she did not feel abdominal pain, and her physical examination was not consistent with that of ileus state at that time. General condition with this case was rather poorer, she was elder, and contrast enhanced CT had no indication because of renal failure. Therefore conservative treatment was chosen. Conservative treatment might be also chosen even if the diagnosis of superior mesenteric artery ischemia was performed at the point of admission. Since performance status was poor with this case and there was no surgical indication.
Conclusion
A case of bowel ischemia during the treatment of AF was reported. When showing smaller mesenteric vein sign like this case, possibility of complication with intestinal ischemia should be considered. Contrast-enhanced CT imaging is useful for its diagnosis when available
REFERENCES
1.
Crawford JD, Perrone KH, Wong VW, et al. A modern series of acute aortic occlusion. J Vasc Surg 2014;59(4):1044–50. [CrossRef]
[Pubmed]

2.
Nakano T, Ito T, Takei T, Takemoto M. Accuracy of the smaller superior mesenteric vein sign for the detection of acute superior mesenteric artery occlusion. Acute Med Surg 2017;5(2):129–32. [CrossRef]
[Pubmed]
3.
Costa AF, Chidambaram V, Lee JJ, Asquith J, Skaff ER, Thipphavong S. Multidetector computed tomography of mesenteric ischaemia. Insights Imaging 2014;5(6):657–66. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Yasuyuki Taooka - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthor declares no conflict of interest.
Copyright© 2020 Yasuyuki Taooka. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}