 |
Case Report
Renal complication due to prune belly syndrome: A case report
1 Medical Sciences Course, Health Sciences School, Faculdade Ceres (FACERES), São José do Rio Preto, SP, Brazil
2 Neurosurgeon, Member of the Brazilian Society of Neurosurgery, Santa Mônica Hospital, Goiânia, GO, Brazil
3 Medical Sciences Course, Health Sciences School, Metropolitan University of Santos, Santos, SP, Brazil
4 Neurosurgeon, PhD in Neurosurgery, Member of the Brazilian Society of Neurosurgery, Professor at Santa Mônica Hospital, Goiânia, GO, Brazil
Address correspondence to:
Pedro Nogarotto Cembraneli
Praça Angelo Testa, nº 40, Jardim das Nações, 12080-050 Taubaté, SP,
Brazil
Message to Corresponding Author
Article ID: 101097Z01PC2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Cembraneli PN, Cavalcante JBDF, Cavalcante RBDF, Ambrogi G, Cavalcante JEDS. Renal complication due to prune belly syndrome: A case report. Int J Case Rep Images 2020;11:101097Z01PC2020.ABSTRACT
Introduction: Prune belly syndrome (PBS) is a congenital disorder characterized by injury or hypoplasia of the abdominal wall musculature, severe urinary tract abnormalities, and bilateral cryptorchidism in males. It has an estimated incidence of 1 in 40,000 live births. Life expectancy is low, and most affected individuals do not survive for more than one year. About 30% of survivors develop chronic renal failure and require a kidney transplant.
Case Report: A male patient, delivered by cesarean section at 39 weeks of gestation, presented with respiratory failure, anuria, flaccid abdomen, bilateral cryptorchidism, and heartbeat with absence of abdominal muscle movements at delivery. Ultrasound of kidneys and urinary tract showed bilateral obstructive hydronephrosis, dilated ureters with tortuous aspect, and bladder partially full with normal wall thickness, suggesting low obstruction. In addition, polycystic kidneys with reduction in renal parenchyma were observed bilaterally. Based on the signs and imaging exam, the patient was diagnosed with PBS. Peritoneal dialysis and ureterostomy were performed. At two years of age, ureteroplasty and orchiopexy were performed, and spontaneous urethral diuresis occurred. After the surgical procedure, the patient underwent hemodialysis for one year before kidney transplant.
Conclusion: Prune belly syndrome is a rare, complex disease with high morbidity and mortality rates. Therefore, early diagnosis before birth during a routine fetal ultrasound or recognition at birth, as well as choice of the most suitable treatment requires greater knowledge of PBS and its complications.
Keywords: Abdominal wall, Cryptorchidism, Prune belly syndrome, Renal insufficiency, Urinary tract
Introduction
Prune belly syndrome (PBS), also known as Eagle-Barret syndrome, triad syndrome, or Obrinsky syndrome, is a congenital disorder with an estimated incidence of 1 in 40,000 live births, and males account for 95% of the cases. It is characterized by absence or hypoplasia of the abdominal wall musculature, severe urinary tract abnormalities, and bilateral cryptorchidism in males [1],[2]. Patients have periumbilical skin folds, giving rise to a wrinkled or prune-like appearance. The testes are close to the ureteral segments at the height of the intra-abdominal iliac vessels. In addition, these individuals may have renal displacement and hydronephrosis [3].
It is considered a multisystemic disease, since it may present with concomitant anomalies, including pulmonary and renal hypoplasia, cardiac and musculoskeletal anomalies, imperforate anus, and varying degrees of intestinal malformation [4],[5]. In addition to the physical problems, this syndrome also negatively affects the emotional, social, and school functioning of these patients, deeply impairing their quality of life [6]. In cases this syndrome affects females, it is considered a pseudosensory syndrome, because they lack the cryptorchidism criterion [5],[7].
Patients with PBS generally have a poor prognosis, and up to 30% of those that suffer from chronic renal failure need kidney transplantation [7]. Therefore, this study aimed to report a case of a 4-year-old patient diagnosed with PBS who underwent a kidney transplant.
Case Report
A male patient, delivered by cesarean section at 39 weeks of gestation, was referred to the neonatal intensive care unit (ICU), since he presented with respiratory failure at the time of delivery, requiring orotracheal intubation. In addition, he had anuria, fluid in the abdomen, bilateral cryptorchidism, and heartbeat with absence of abdominal muscle movements. Family members reported that no complications were noticed during prenatal care, except in the last trimester, when oligohydramnios was diagnosed.
In the neonatal ICU, ultrasound of kidneys and urinary tract revealed bilateral obstructive hydronephrosis, dilated tortuous ureters, and bladder partially full with normal wall thickness, suggesting low obstruction. Moreover, polycystic kidneys with reduction in renal parenchyma were observed bilaterally. Therefore, a suprapubic cystostomy was indicated and performed. Based on the signs and imaging exam, the patient was diagnosed with PBS.
During the first months of life, he had recurrent urinary tract infections, requiring the use of an oral outpatient protocol with cephalexin. At eight months of age, laboratory tests showed chronic renal failure and anemia, and the patient needed a blood transfusion. During this procedure, he had urticarial plaques and the transfusion was suspended. The child was treated with erythropoietin, hixizine, and prednisone.
He underwent a urethrocystography that identified the partially filled, elongated, thick-walled bladder, but did not identify the ureters. In addition, he had episodes of hyperkalemia and uremia. A Tenckhoff catheter was placed and peritoneal dialysis and ureterostomy were scheduled. Three months later, he underwent bilateral nephrostomy, and since the left kidney presented ureteropelvic junction stenosis, it was resected and sent for analysis. After that, the patient started home peritoneal dialysis five times a day.
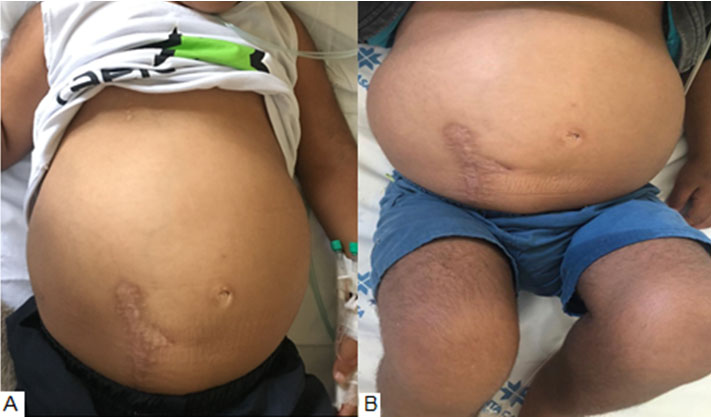
At two years of age, ureteroplasty and orchiopexy were performed, and spontaneous urethral diuresis occurred. After this surgical procedure, he underwent hemodialysis for one year before a kidney transplant was performed. Currently, at four years of age, he presents with distended abdomen (Figure 1), hypertrichosis, and cushingoid facies (Figure 2). The patient takes doxazosin mesylate, cyclosporine, mycophenolate mofetil, amlodipine, prednisone, and bactrim. He continues being followed up as a pediatric nephrology outpatient.

Discussion
Prune belly syndrome is characterized by a classic triad: deficient or absent abdominal muscles, urinary tract abnormalities, and bilateral cryptorchidism [5],[8]. The genetic basis of this condition remains unknown. However, some authors affirm that it is the result of an abnormal development of the middle and lateral plate mesoderm during the third week of gestation, responsible for the formation of the urinary tract, kidneys, and abdominal wall [9],[10],[11].
Life expectancy of PBS patients is low, and up to 30% of them do not survive for more than one year. Neonatal mortality rate reaches 23%, 20% are stillborn, and 43% are premature [12].
Laxity of the abdominal wall musculature can lead to several effects, such as difficulty in urinating, impaired bowel movements, and postural changes. In addition, due to the absence of intra-abdominal pressure, the individual is more prone to develop respiratory tract infections secondary to impaired cough mechanism, and to chronic constipation because of ineffective Valsalva maneuver [12],[13]. Another frequent symptom is recurrent urinary tract infections due to incomplete bladder emptying leading to urinary stasis [14].
The diagnosis of PBS can be made using intrauterine ultrasound, usually in the 13th week of gestation. In general, ultrasound findings include bulging abdomen, lack of abdominal muscles, dilated bladder and ureters, hydronephrosis, polycystic or dysplastic kidneys, fetal ascites, oligohydramnios, and hypoplastic lungs [15],[16]. Nevertheless, if it is not diagnosed during pregnancy, at birth the above mentioned triad helps the clinical identification of PBS.
The management of PBS depends on the severity of the clinical findings. In some cases, prenatal intervention using vesicoamniotic shunt therapy is required to repair severe obstructive uropathies, which otherwise lead to oligohydramnios and pulmonary hypoplasia [17],[18]. After birth, it is generally necessary to perform a surgical procedure, such as a button cystostomy for adequate bladder drainage to prevent complications [19]. For patients with end-stage renal disease, hemodialysis or continuous peritoneal dialysis is indicated before kidney transplantation [20],[21],[22],[23].
In male subjects, Fowler-Stephens orchiopexy should not be delayed until adolescence, so that spontaneous onset of puberty can be reached, resulting in satisfactory sexual function in adulthood [24]. Additionally, in many cases, abdominoplasty is performed for aesthetic or psychosocial reasons, aiming to improve intra-abdominal pressure. As a consequence, pulmonary, intestinal, bladder, and postural functions are also improved [6],[25],[26],[27],[28].
Conclusion
Prune belly syndrome is a rare, complex disease with high morbidity and mortality rates. For a better prognosis, PBS diagnosis should be made early, preferably in utero. Physicians and pregnant women should be alerted to the importance of prenatal care, inasmuch as the early detection and identification of congenital abnormalities allows health professionals to define proper treatment. Further studies on the pathogenesis, diagnosis, and management of patients with PBS are required to acquire greater knowledge of this disease and its complications since the literature on the syndrome is scarce.
REFERENCES
1.
Lloyd JC, Wiener JS, Gargollo PC, Inman BA, Ross SS, Routh JC. Contemporary epidemiological trends in complex congenital genitourinary anomalies. J Urol 2013;190(4 Suppl):1590–5. [CrossRef]
[Pubmed]

2.
Seidel NE, Arlen AM, Smith EA, Kirsch AJ. Clinical manifestations and management of prune-belly syndrome in a large contemporary pediatric population. Urology 2015;85(1):211–5. [CrossRef]
[Pubmed]
3.
Carvalho NDS, Cavachini C, Dudus MM. Sìndrome de prune belly. Resid Pediatr 2018;8(1):45–7.
4.
Jennings RW. Prune belly syndrome. Semin Pediatr Surg 2000;9(3):115–20. [CrossRef]
[Pubmed]
5.
Routh JC, Huang L, Retik AB, Nelson CP. Contemporary epidemiology and characterization of newborn males with prune belly syndrome. Urology 2010;76(1):44–8. [CrossRef]
[Pubmed]
6.
Arlen AM, Kirsch SS, Seidel NE, Garcia-Roig M, Smith EA, Kirsch AJ. Health-related quality of life in children with prune-belly syndrome and their caregivers. Urology 2016;87:224–7. [CrossRef]
[Pubmed]
7.
Behrman RE, Kliegman RM, Jenson HB. Nelson: Tratado de Pediatria. 19ed. Rio de Janeiro: Elsevier; 2014.
8.
Osler W. Congenital absence of the abdominal muscles with distended and hypertrophied urinary bladder. Bull Johns Hopkins Hosp 1901;12:331–3.
9.
Bomfim KB, da Silva-Hamu TCD. Aspectos clìnicos da sìndrome de prune belly: Revisão de literatura. Rivista Movimenta 2013;6(4):596–605.
10.
Murray PJ, Thomas K, Mulgrew CJ, Ellard S, Edghill EL, Bingham C. Whole gene deletion of the hepatocyte nuclear factor-1beta gene in a patient with the prune-belly syndrome. Nephrol Dial Transplant 2008;23(7):2412–5. [CrossRef]
[Pubmed]
11.
Haeri S, Devers PL, Kaiser-Rogers KA, et al. Deletion of hepatocyte nuclear factor-1-beta in an infant with prune belly syndrome. Am J Perinatol 2010;27(7):559–63. [CrossRef]
[Pubmed]
12.
Bogart MM, Arnold HE, Greer KE. Prune-belly syndrome in two children and review of the literature. Pediatr Dermatol 2006;23(4):342–5. [CrossRef]
[Pubmed]
13.
Woods AG, Brandon DH. Prune belly syndrome. A focused physical assessment. Adv Neonatal Care 2007;7(3):132–43. [CrossRef]
[Pubmed]
14.
Herman TE, Siegel MJ. Prune belly syndrome. J Perinatol 2009;29(1):69–71. [CrossRef]
[Pubmed]
15.
Ferreira ACR, Santos CCT, Miranda CSSP, Silva KJM, Lopes VC, Guilherme IS. Sìndrome de prune belly-relato de caso. Rev Cient Sena Aires 2017;6(2):134–7.
16.
Garcia-Roig ML, Grattan-Smith JD, Arlen AM, Smith EA, Kirsch AJ. Detailed evaluation of the upper urinary tract in patients with prune belly syndrome using magnetic resonance urography. J Pediatr Urol 2016;12(2):122.e1–7. [CrossRef]
[Pubmed]
17.
Leeners B, Sauer I, Schefels J, Cotarelo CL, Funk A. Prune-belly syndrome: Therapeutic options including in utero placement of a vesicoamniotic shunt. J Clin Ultrasound 2000;28(9):500–7. [CrossRef]
[Pubmed]
18.
Biard JM, Johnson MP, Carr MC, et al. Long-term outcomes in children treated by prenatal vesicoamniotic shunting for lower urinary tract obstruction. Obstet Gynecol 2005;106(3):503–8. [CrossRef]
[Pubmed]
19.
Milliken I, Munro NP, Subramaniam R. Cystostomy button for bladder drainage in children. J Urol 2007;178(6):2604–6. [CrossRef]
[Pubmed]
20.
Fusaro F, Zanon GF, Ferreli AM, et al. Renal transplantation in prune-belly syndrome. Transpl Int 2004;17(9):549–52. [CrossRef]
[Pubmed]
21.
Kamel MH, Thomas AA, Al-Mufarrej FM, O'Kelly P, Hickey DP. Deceased-donor kidney transplantation in prune belly syndrome. Urology 2007;69(4):666–9. [CrossRef]
[Pubmed]
22.
Djakovic N, Wagener N, Adams J, et al. Intestinal reconstruction of the lower urinary tract as a prerequisite for renal transplantation. BJU Int 2009;103(11):1555–60. [CrossRef]
[Pubmed]
23.
Hatch DA, Koyle MA, Baskin LS, et al. Kidney transplantation in children with urinary diversion or bladder augmentation. J Urol 2001;165(6 Pt 2):2265–8. [CrossRef]
[Pubmed]
24.
Patil KK, Duffy PG, Woodhouse CR, Ransley PG. Long-term outcome of Fowler-Stephens orchiopexy in boys with prune-belly syndrome. J Urol 2004;171(4):1666–9. [CrossRef]
[Pubmed]
25.
Dénes FT, Lopes RI, Oliveira LM, Tavares A, Srougi M. Modified abdominoplasty for patients with the prune belly syndrome. Urology 2014;83(2):451–4. [CrossRef]
[Pubmed]
26.
Smith EA, Srinivasan A, Scherz HC, Tracey AJ, Broecker B, Kirsch AJ. Abdominoplasty in prune belly syndrome: Modifications in Monfort technique to address variable patterns of abdominal wall weakness. J Pediatr Urol 2017;13(5):502.e1–502.e6. [CrossRef]
[Pubmed]
27.
Franco I. Laparoscopic assisted modification of the firlit abdominal wall plication. J Urol 2005;174(1):280–3. [CrossRef]
[Pubmed]
28.
Dénes FT, Arap MA, Giron AM, Silva FA, Arap S. Comprehensive surgical treatment of prune belly syndrome: 17 years' experience with 32 patients. Urology 2004;64(4):789–93. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Pedro Nogarotto Cembraneli - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Julia Brasileiro de Faria Cavalcante - Conception of the work, Design of the work, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Renata Brasileiro de Faria Cavalcante - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Gabriel Ambrogi - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
José Edison da Silva Cavalcante - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Pedro Nogarotto Cembraneli et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}