 |
Case Report
Pleural drop-metastasis five years post-thymectomy manifesting with myasthenia gravis
1 Intern, Florida Lung Asthma and Sleep Specialists, Orlando, Florida, USA
2 Attending Physician, Florida Lung Asthma and Sleep Specialists, Orlando, Florida, USA
Address correspondence to:
Fortune O Alabi
(MD, FABSM, FCCP), Intern, Florida Lung Asthma and Sleep Specialists, Orlando, Florida,
USA
Message to Corresponding Author
Article ID: 101060Z01CA2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Alabi CO, Basso RG, Alabi FO. Pleural dropmetastasis five years post-thymectomy manifesting with myasthenia gravis. Int J Case Rep Images 2019;10:101060Z01CA2019.ABSTRACT
Introduction: Thymomas are the most common tumors in the anterior mediastinum. Intrathoracic recurrence of thymomas after initial resection is common and mostly seen in patients with advanced Masaoka stage. A number of paraneoplastic syndromes can be associated with thymoma, but myasthenia gravis (MG) is the most common. A total radical thymectomy often leads to a resolution of MG in a considerable number of patients. However, MG relapse post-thymectomy can occur whether there is a recurrence of the thymoma or not. In this case report, a patient presented with MG five years after radical removal of a thymoma which was not associated with MG before his surgery.
Case Report: A 47-year-old male while on admission for acute meningitis was incidentally found to have a mediastinal mass on a chest X-ray and then confirmed by computed tomography (CT) of the chest. The mass was about 5 × 3 cm in size and located in the left perivascular space of his mediastinum. A biopsy of the mass obtained by Chamberlain procedure confirmed the presence of invasive thymoma (WHO type B2). He had no features suggestive of associated paraneoplastic syndrome. The thymoma was subsequently resected and found to be Masaoka stage 3. Postoperative radiotherapy was suggested to the patient, but he declined it. Five years later, the patient presented with ptosis, intermittent generalized muscle weakness with occasional shortness of breath and was diagnosed with MG with positive acetylcholine receptor antibodies. He was treated with pyridostigmine and plasmapheresis. A minimally heterogenous 10.6 × 4.4 cm mass was found within the posteromedial aspect of the pleural reflection of his left lower lung lobe on chest CT scan with contrast. A CT-guided biopsy of the mass was performed which confirmed the recurrence of the invasive thymoma with pathology report histologically similar to the previously resected thymoma. The patient was diagnosed with recurrence of invasive thymoma by pleural drop-metastasis and was managed by radiation therapy.
Conclusion: Myasthenia gravis can manifest on recurrence of thymoma in a patient post-thymectomy even though there was no MG associated with the initial thymoma.
Keywords: Myasthenia gravis, Pleural metastasis, Post-thymectomy, Thymoma
Introduction
Thymoma represents up to 40–50% of all anterior mediastinal tumors and even though a true thymoma usually has cytologically benign elements. It can invade local anatomical structures and can have intrathoracic recurrence after resection [1],[2]. The recurrence of invasive thymoma has a predilection for the pleural surface and the risk of recurrence is higher in patients who underwent biopsy prior to resection [3],[4].
Myasthenia gravis is the most common paraneoplastic syndrome in thymoma patients seen in about 24.5–40% of cases whereas only about 15–20% of MG patients have thymoma [5]. A total radical thymectomy often leads to a resolution of MG in a considerable number of patients who have MG associated with thymoma, but MG relapse post-thymectomy can occur whether there is a recurrence of the thymoma or not [6].
This is a report of a patient who presented with MG five years after total radical removal of a thymoma which was not associated with myasthenia gravis preresection.
Case Report
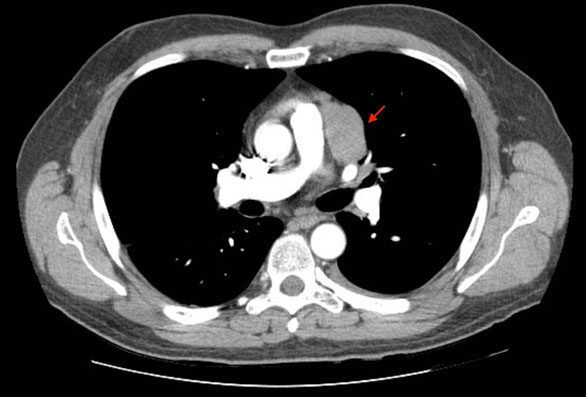
A 47-year-old male patient while on admission for acute meningitis had a chest X-ray done which showed a left mediastinal shadow. He was treated for his infection and had a follow-up chest CT with contrast which confirmed the presence of a wellcircumscribed 5 × 3 cm mass without calcifications in the left perivascular space of his mediastinum (Figure 1). The mass was suspected to either be a lymphoma or thymoma. A biopsy was obtained via Chamberlain procedure and the pathology showed invasive thymoma (WHO type B2).
He had a radical en bloc total thymectomy with resection of part of the pericardium, the left phrenic nerve was also harvested during the procedure and the pathology showed invasive thymoma (Masaoka Stage 3, WHO type B2). Postoperative radiotherapy (PORT) was recommended, which the patient declined.
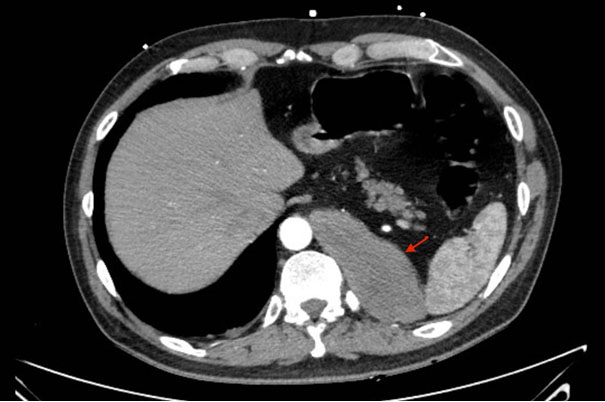
Five years later he presented with a history of ptosis, intermittent muscle weakness, and occasional shortness of breath. Acetylcholine receptor antibody test came back positive and the diagnosis of MG was made. Chest CT with contrast showed no definitive soft tissue density within the mediastinum but a minimally heterogenous mass was found within the left lower lung lobe in the posteromedial pleural reflection measuring 10.6 × 4.4 cm on axial image (Figure 2).
A biopsy of the left lower pleural base mass found invasive thymoma histologically consistent with the grade of the initial lesion and a diagnosis of pleural drop-metastasis of recurrent invasive thymoma was made. The patient was treated with plasmapheresis and pyridostigmine for the MG and the left lower mass was radiated.
The medical history of our patient before presenting with features of MG included bronchiectasis with Mycobacterium avium complex, which was treated with triple therapy. He had multiple bouts of airway infections with Pseudomonas aeruginosa and Mycobacterium massiliense colonization. He was found to be lymphopenic in all his admission charts, but human immunodeficiency virus (HIV) test was negative and lymphocyte subtype testing was not performed. The association of thymoma with hypogammaglobulinemia is well known and called Good’s syndrome. However, he had normal immunoglobulin levels, but specific antibody deficiency was not excluded because antibody response to vaccination was not performed. Therefore, we could not reach a definitive diagnosis of immunodeficiency despite his history of recurrent bacterial infections and nontuberculous mycobacterium infections that were difficult to eradicate.
Discussion
A thymoma can be an incidental finding on imaging, present with local thoracic pressure symptoms, or symptoms of paraneoplastic syndromes known to be associated with it. Some common paraneoplastic syndromes that can be associated with thymoma include:MG, pure red cell aplasia, and hypogammaglobulinemia [7]. Most thymomas are asymptomatic and discovered incidentally as an anterior mediastinal mass, just like in this patient. In cases where the CT scan shows a mass that looks suspicious for thymoma and appears amenable to complete surgical resection, the next step should be a total radical thymectomy without any need for biopsy. A possible sequela of the biopsy is seeding of the needle tract, pleura, mediastinal space, and even the chest wall by cells of the tumor thereby increasing the risk of recurrence [8],[9].
The patient has cortical thymoma with many lymphocytes and unhealthy thymus cells (WHO type B2) with evidence of macroscopic invasion into adjacent organs (Masaoka stage 3). High stage thymoma has been said to strongly predict thymoma recurrence postresection with stage 3 thymoma having a 26.8% chance of recurrence after resection [10]. Other factors that could have caused the recurrence in this patient include the possibility of shedding tumor cells into surrounding structures or even the pleural space when the capsule of the tumor was bridged for tissue biopsy or the fact that he declined postoperative radiotherapy which has been linked to improved overall survival in patients with Masaoka stage 3 and 4 [9],[11].
A case similar to this was published by Heyman et al. about a patient who had a recurrent thymoma secondary to pleural implant three years after radical thymectomy [12]. The patient initially presented with symptoms of MG before the mediastinal mass was found. In our case, the patient did not have MG initially but only presented with MG when he had thymoma recurrence. To our knowledge, this is the first published case where MG occurred with a histologically diagnosed recurrent thymoma despite not being present clinically during the initial presentation.
Conclusion
Myasthenia gravis can manifest on recurrence of thymoma in a patient post-thymectomy even though there was no MG associated with the initial thymoma.
REFERENCES
1.
Singh G, Rumende CM, Amin Z. Thymoma: Diagnosis and treatment. Acta Med Indones 2011;43(1):74–8.
[Pubmed]

2.
Donoiu I, Radu RI, Giucă A, Popescu M, Ionescu DD. Invasive thymoma. Rom J Morphol Embryol 2010;51(3):573–5.
[Pubmed]
3.
Detterbeck FC, Parsons AM. Thymic tumors. Ann Thorac Surg 2004;77(5):1860–9. [CrossRef]
[Pubmed]
4.
Regnard JF, Zinzindohoue F, Magdeleinat P, Guibert L, Spaggiari L, Levasseur P. Results of re-resection for recurrent thymomas. Ann Thorac Surg 1997;64(6):1593–8. [CrossRef]
[Pubmed]
5.
Evoli A, Lancaster E. Paraneoplastic disorders in thymoma patients. J Thorac Oncol 2014;9(9 Suppl 2):S143–7. [CrossRef]
[Pubmed]
6.
Uzawa A, Kanai T, Oda F, et al. Frequency and features of myasthenia gravis developing after thymectomy. Eur J Neurol 2019. [CrossRef]
[Pubmed]
7.
Briones J, Iruretagoyena M, Galindo H, et al. Thymoma associated with hypogammaglobulinaemia and pure red cell aplasia. Ecancermedicalscience 2013;7:364. [CrossRef]
[Pubmed]
8.
Nagasaka T, Nakashima N, Nunome H. Needle tract implantation of thymoma after transthoracic needle biopsy. J Clin Pathol 1993;46(3):278–9. [CrossRef]
[Pubmed]
9.
Kattach H, Hasan S, Clelland C, Pillai R. Seeding of stage I thymoma into the chest wall 12 years after needle biopsy. Ann Thorac Surg 2005;79(1):323–4. [CrossRef]
[Pubmed]
10.
Bae MK, Lee CY, Lee JG, et al. Predictors of recurrence after thymoma resection. Yonsei Med J 2013;54(4):875–82. [CrossRef]
[Pubmed]
11.
Lim YJ, Kim E, Kim HJ, et al. Survival impact of adjuvant radiation therapy in Masaoka stage II to IV thymomas: A systematic review and meta-analysis. Int J Radiat Oncol Biol Phys 2016;94(5):1129–36. [CrossRef]
[Pubmed]
12.
Heyman SR, De Raeve H, Mercelis R, De Pooter C, Van Schil P. Recurrent myasthenia gravis due to a pleural implant 3 years after radical thymectomy. Ann Thorac Surg 2008;86(1):299–301. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Christopher O Alabi - Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Rafaela G Basso - Conception of the work, Design of the work, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fortune O Alabi - Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Christopher O Alabi et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}