 |
Case Report
Spontaneous trans-visceral migration and intestinal obstruction due to a textiloma: A case report
1 Department of Surgery, University of Abuja Teaching Hospital Gwagwalada, Nigeria
2 Department of Surgery, College of Health Sciences University of Abuja, Gwagwalada, Nigeria
3 Department of Family Medicine, Asokoro District Hospital Abuja, Nigeria
Address correspondence to:
Ifeanyi Charles Umoke
Department of Surgery, University of Abuja Teaching Hospital Gwagwalada,
Nigeria
Message to Corresponding Author
Article ID: 101026Z01IU2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Umoke IC, Stephen GE, Henrietta UN, Abubakar HK. Spontaneous trans-visceral migration and intestinal obstruction due to a textiloma: A case report. Int J Case Rep Images 2019;10:101026Z01IU2019.ABSTRACT
Introduction: Retained surgical sponge, otherwise called, gossypiboma, textiloma or gauzioma is a rare but the most frequently encountered retained foreign body after abdominal surgery. It is under reported in medical literature due to the medico-legal implications. The incidence has been put at 1:3000 to 1:100 surgeries by one series while another series put it at 1:5500 surgeries. Nonetheless, it is a condition with considerable morbidity and a mortality rate of about 10%.
Case Report: We report a case of spontaneous transmural migration of a textiloma with consequent subacute intestinal obstruction in a 31-year-old woman who had caeserean section for poor progress of labour six weeks prior to onset of features of intestinal obstruction.
Conclusion: Various methods have been devised by various institutions to reduce the incidence of retained surgical sponges the most effective being the radio-frequency system. However, the availability of the radio-frequency system may be low in low resource settings leaving the option of diligently utilizing the WHO safety check list for operation theatres as an alternative to curbing this distressing condition which is completely avoidable.
Keywords: Gossypiboma, Intestinal obstruction, Trans-visceral migration
Introduction
Retained gauze piece also called gossypiboma/ gauzioma/ textiloma is a rare surgical complication [1]. It is the most frequently encountered retained surgical foreign body, as there have been cases of other retained surgical foreign bodies such as needles and other instruments [2]. It is not diligently reported because of the medico-legal implications. Thus, the incidence is much higher than is reported in medical literature [3]. Some series put the incidence between 1 in 1000 to 1500 surgeries [4] while another series put the incidence at 1 in 5500 to 18,760 operations [5]. As a foreign body, it may cause a foreign body granuloma, pelvic abscess, abdominal pain, fistula formation, or the rare complication of transmural migration through the bowel wall [3]. Only a few cases of transmural migration through the bowel wall have been reported in medical literature [6].
Retained surgical sponge/gauze, RSG, may present early or may remain silent for years before symptoms evolve. It is an avoidable complication with considerable morbidity and mortality rate which has been put as high as 10% [4].
Case Report
A 31-year-old woman who presented in the Emergency Room on account of recurrent colicky abdominal pain from 10 months. Pain was of insidious onset and located in the periumbilical and left lumbar areas. There was associated episodes of billous vomitting. There was intermittent episodes of loose stools. No abdominal distention. There was history of significant weight loss. She had emergency caesarean section six weeks prior to onset of abdominal pain due to poor progression of labour. Examination revealed a young woman who was wasted and mildly dehydrated. Vitals were stable and normal. Abdominal examination showed a flat abdomen with a transverse suprapubic surgical scar. There was tenderness in the umbilical and left lumbar areas. There was no palpable intra-abdominal masses. Bowel sounds were hyperactive. Digital rectal examination was unremarkable.
Investigations
- Abdomino-pelvic ultrasound scan showed a well-defined concentric mass with alternating hypodensity in the left flank giving a characteristic target and reniform appearance on longitudinal and transverse views measuring 4.9x4.6 cm. There was hyperactivity of the adjacent bowel with mild dilatation.
- Plain abdominal X-rays showed mild dilatation of the large bowel.
- Colonoscopy was unremarkable.
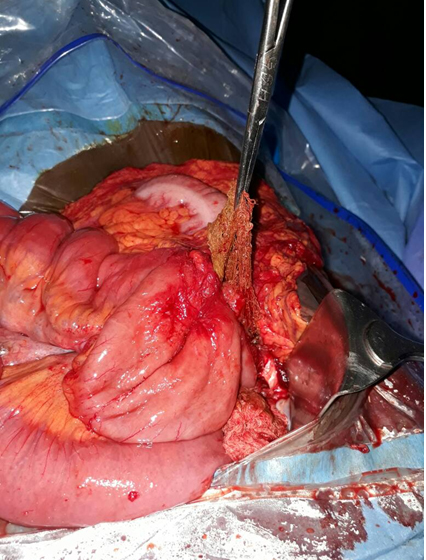
A diagnosis of adhesive intestinal obstruction was made and non-operative management instituted. However, this was suspended with non-resolution of symptoms. A laparotomy was done. Intra-operative findings included a jejunal portion of the small gut which was attached by adhesions to the sigmoid colon and the left anterio-lateral part of the abdominal wall from where a thick cord-like structure with a bulbous end which was partially occluding the lumen, was palpated intraluminally and extended for about 40 cm distally towards the ileum, giving a plicated appearance to the involved segment of the gut which was dilated proximally. In an attempt to seperate the adhesions, the jejunum was iatrogenically opened revealing an intraluminal gauze band with faecal concretions. The proximal end of the gauze which was still extraluminal was firmly attached to the sigmoid colon accounting for the jejunal tethering as described above (Figure 1), (Figure 2), (Figure 3). Both the jejunum and sigmoid were resected at the affected areas and primary end to end anastomoses was done in a single layer. Patient had a minor anastomotic leakage on the eighth postoperative day that sealed on the tenth post-operative day. She was discharged on the twelfth post-operative day.


Discussion
Two types of foreign body reactions usually result from RSS. An asceptic fibrinous response which can form either a granuloma or pseudotumor. This usually follows a silent course. The other is an exudative response which leads to abscess formation. RSS may remain silent for months or even years or result in such complications as intestinal obstruction, fistula formation, peritonitis, spontaneous expulsion, transmural migration into the small bowel, stomach, large bowel, urinary bladder [7],[8] or erode into a neighboring blood vessel. Migration into the intestinal lumen may occur without apparent opening in the intestinal wall. Our patient had a transmural migration into the bowel lumen.
Defense mechanisms in the peritoneal cavity utilized the weak resistance presented by the intestinal tract to try and expel a RSS [8],[9]. Successful expulsions through the rectum of sponges small enough to pass through the ileocaecal valve or by direct penetration of the colorectum have been reported [8],[9].
Various hypotheses have been put forward to explain the mechanism of transmural migration. The first stage is a foreign body reaction when the sponge is walled off by omentum and loops of bowel. This is followed by secondary infection when the cotton filament reach the intestinal lumen following cytolysis. Invasion of the sponge into the lumen occurs at the stage of mass formation. Remodeling is the last stage when a fibrotic scar is formed at the site of the migration [10].
Patil and colleagues opined that pressure necrosis of the intestinal wall, which may be partial or complete, by an increased pressure of the intra-abdominal mass will lead to a fistula or intestinal obstruction [11].
Some risk factors for RSS have been identified and include emergency, prolonged surgical procedure, unplanned change in the course of a surgical procedure, involvement of more than one surgical team and patients with higher body mass index [1],[12].
Diagnosis of RSS can be made with the aid of X-rays if there is a radio-opaque marker in the sponge. On ultrasonography, RSS are echogenic and create an intensive and sharply demarcated acoustic shadow. On CT scan, a low density mass with prominent ring enhancement in addition to a spongiform bubble may suggest a RSS granuloma. This is also known as the whirl sign. MRI shows a mass with a capsule showing high intensity signal [13]. In an attempt to account for surgical materials that are placed in the body, different hospitals employ different methods. These include meticulous counting and routine use of surgical textile material impregnated with a radio-opaque markers, in addition to thorough exploration of the surgical sites at the conclusion of operation. These should reduce the incidence of RSS. However 88% cases of RSS still occur after ‘correct’ surgical counts, indicating that mechanical counting alone is not a reliable mechanism in eliminating RSFB [12].
Currently, a specialized radio-opaque frequency system consisting of radio-frequency detector and radio-frequency labeled sponges has been designed and being utilized to eliminate the human error factor. The sensitivity and specificity of this system has been shown to be much higher than those of surgical sponge counts or the published findings on the intra-operative radiographs to identify retained surgical sponges [14].
Conclusion
Retained surgical foreign body (RSFB), a rare complication of surgery is still under reported. This is due largely to the huge medico-legal implications. A more advanced technological method that employs a radio-frequency system has shown superior results to any other means hitherto in detecting and reducing this complication. However, in a resource-constrained environment like ours, the diligent application of the WHO safety checklist for operation theatres is still a useful adjunct in the prevention of such complication.
REFERENCES
1.
Stawicki SP, Evans DC, Cipolla J, et al. Retained surgical foreign bodies: A comprehensive review of risks and reventive strategies. Scand J Surg 2009;98(1):8–17. [CrossRef]
[Pubmed]

2.
Lu YY, Cheung YC, Ko SF, Ng SH. Calcified reticular ring sign: A characteristic feature of gossypiboma on computed tomography. World J gastroenterol 2005;11(31):4927–9. [CrossRef]
[Pubmed]
3.
Ahmad G, Attiq-ur-Rehman S, Anjum MZ. Retained sponge after abdominal surgery. J Coll Physicians Surg Pak 2003;13(11):640–3.
[Pubmed]
4.
Hariharan D, Lobo DN. Retained surgical sponges, needles and instruments. Ann R Coll Surg Engl 2013;95(2):87–92. [CrossRef]
[Pubmed]
5.
Cima RR, Kollengode A, Garnatz J, Storsveen A, Weisbrod C, Deschamps C. Incidence and characteristics of pontential and actual retained foreign object events in surgical patients. J Am Coll Surg 2008;207(1):80–7. [CrossRef]
[Pubmed]
6.
Grassi N, Cipolla C, Torcivia A, et al. Trans-visceral migration of retained surgical gauze as a cause of intestinal obstruction: A case report. J Med Case Rep 2008;2:17. [CrossRef]
[Pubmed]
7.
Sarda AK, Pandey D, Neogi S, Dhir U. Postoperative complications due to a retained surgical sponge. Singapore Med J 2007;48(6):e160–4.
[Pubmed]
8.
Zantvoord Y, vander Weiden RM, van Hooff MH. Transmural migration of retained surgical sponges: A systematic review. Obstet Gynaecol Surv 2008;63(7):465–71. [CrossRef]
[Pubmed]
9.
Godara R, Marwah S, Karwasra RK, Goel R, Sen J, Singh R. Spontaneous transmural migration of surgical sponges. Asia J Surg 2006;29(1):44–5. [CrossRef]
[Pubmed]
10.
Wattanasirichaigoon S. Transmural migration of retained surgical sponges into the intestinal lumen: An experimental study. J Med Assoc Thai 1996;79(7):415–22.
[Pubmed]
11.
Patil KK, Patil SK, Gorad KP, Panchal AH, Arora SS, Gautam RP. Intraluminal migration of surgical sponge: Gossypiboma. Saudi J gastroenterol 2010;16(3):221–2. [CrossRef]
[Pubmed]
12.
Gawande AA, Struddert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factor for retained instruments and sponges after surgery. N Engl J Med 2003;348(3):229–35. [CrossRef]
[Pubmed]
13.
Manzella A, Filho PB, Albuquerque E, Farias F, Kaercher J. Imaging of gossypibomas: Pictoral review. AJR Am J Roentgenol 2009;193(6 Suppl):S94–101. [CrossRef]
[Pubmed]
14.
Steelman VM, Alasagheirin MH. Assessment of radiofrequency device senstivity for the detection of retained surgical sponges in patients with morbid obesity. Arch Surg 2012;147(10):955–60. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ifeanyi Charles Umoke - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Garba E. Stephen - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Umoke Nnenna Henrietta - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hamza K. Abubakar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this study.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Ifeanyi Charles Umoke et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}