 |
Clinical Image
A rare case of steroid responsive Torsades de pointes
1 Chair, Department of Medicine, Moffitt Cancer Center, Tampa, Florida, USA
2 Academic Hospitalist, Department of Medicine, James A. Haley VA Hospital, Tampa, Florida, USA
Address correspondence to:
Asha Ramsakal
DO, MBS, FACP, 12902 USF Magnolia Drive, Tampa, Florida 33612,
USA
Message to Corresponding Author
Article ID: 101017Z01AR2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Ramsakal A, Dass VL. A rare case of steroid responsive Torsades de pointes. Int J Case Rep Images 2019;10:101017Z01AR2019.ABSTRACT
No Abstract
Keywords: Myocarditis, Pembrolizumab, Steroids, Torsades de pointe
Case Report
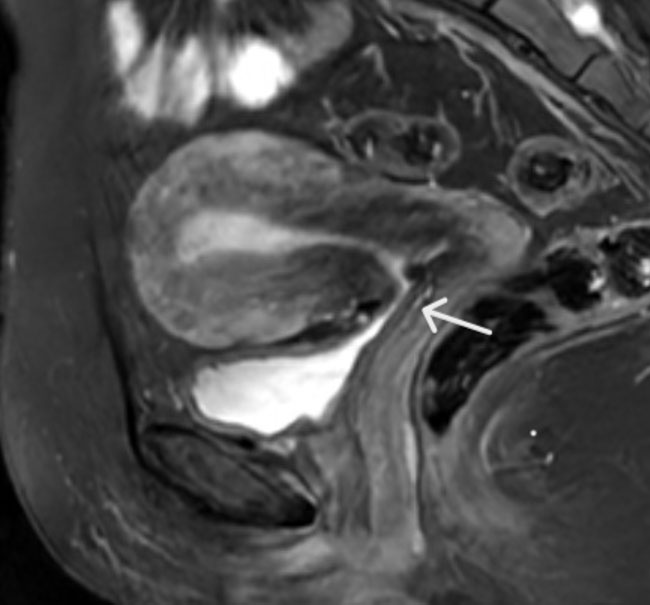
A 37-year-old female with sarcoma on pembrolizumab experienced lightheadedness during hospitalization. Telemetry revealed Torsades de pointes (TdP) that lasted 3.8 seconds (Figure 1). Her potassium, magnesium and troponin were normal. Admission EKG was sinus bradycardic at 44 bpm with a QTc of 478 ms. Cardiac MRI revealed subtle focal myocardial edema in the left ventricular septal wall suspicious for mild myocarditis likely secondary to pembrolizumab. The patient was given 2 grams of intravenous magnesium sulfate and initiated on methylprednisolone 1 mg/kg intravenously daily. She had no further lightheadedness or episodes of TdP. She was discharged on a course of tapering oral prednisone. Patient was also instructed to avoid all QT prolonging medications. Her pembrolizumab was discontinued. The patient was still asymptomatic at follow-up in five weeks and her QTc had decreased to 388 ms.

Discussion
Pembrolizumab is a highly selective programmed cell death receptor-1 (PD-1) blocking antibody which reverses T-cell suppression and in doing so promotes antitumor responses [1]. The incidence of myocarditis is rare (<1%). The most common etiology of TdP is QT prolonging medications [2]. Other risk factors include bradycardia, electrolyte abnormalities (hypokalemia, hypomagnesemia and hypocalcemia), female sex, underlying structural heart disease and advanced age. Patients with multiple risk factors present with the greatest risk [3]]. Our patient was female, had baseline bradycardia at 44 bpm and was on ondansetron plus metoclopramide both of which can prolong the QT interval.
The key to management of TdP in stable patients is to identify and treat the potentially reversible risk factors. In our patient’s case, it was to discontinue the pembrolizumab, ondansetron and metoclopramide. Another therapy with proven benefit is intravenous magnesium sulfate even in patients with normal magnesium levels [4]. In addition, the initial management of immune mediate myocarditis is a course of steroids [5]. Our patient responded quite favorably to methylprednisolone 1 mg/kg intravenously daily initially and then was successfully transitioned to an oral prednisone taper without further lightheadedness or episodes of TdP.
Conclusion
Pembrolizumab is a programmed cell death receptor-1 blocking antibody. To our knowledge this is the first reported case of Torsades-de-pointes associated with pembrolizumab immune-mediated myocarditis that was successfully responsive to steroids. The authors recommend telemetry monitoring of patients on pembrolizumab and avoidance of concomitant QT prolonging medications. If patients develop pembrolizumab-induced TdP, intravenous magnesium sulfate is indicated even in the absence of hypomagnesemia plus prednisone 1 mg/kg daily with a subsequent taper.
REFERENCES
1.
Robert C, Ribas A, Wolchok JD, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: A randomised dose-comparison cohort of a phase 1 trial. Lancet 2014;384(9948):1109–17. [CrossRef]
[Pubmed]

2.
Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart 2003;89(11):1363–72.
[Pubmed]
3.
Drew BJ, Ackerman MJ, Funk M, et al. Prevention of torsades de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation 2010;121(8):1047–60. [CrossRef]
[Pubmed]
4.
Tzivoni D, Banai S, Schuger C, et al. Treatment of torsade de pointes with magnesium sulfate. Circulation 1988;77(2):392–7.
[Pubmed]
5.
Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J Clin Oncol 2018;36(17):1714–68. [CrossRef]
[Pubmed]
SUGGESTED READING
SUPPORTING INFORMATION
Author Contributions
Asha Ramsakal - Conception of the work, Design of the work, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Vadin Lall Dass - Conception of the work, Design of the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guarantor of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Asha Ramsakal et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


{kind=link}
{kind=link}
{kind=link}
{kind=link}